
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Delayed cerebral ischemia after coil embolization of an
unruptured giant intracranial aneurysm: A case report
*Corresponding Author : Wang yan
The Center of Emergency and Disaster Medicine, the Seventh Affiliated Hospital, Sun Yat-sen University, Zhenyuan Road 628, Guangming District, Shenzhen, 518000, China.
Email: wangyan@sysush.com
Received : Apr 04, 2023
Accepted : Apr 24, 2023
Published : May 01, 2023
Archived : www.jcimcr.org
Copyright : © Yan W (2023).
Keywords: Unruptured aneurysm; Coil embolization; Delayed cerebral ischemia; Complication.
Citation: Wang yan, Delayed cerebral ischemia after coil embolization of an unruptured giant intracranial aneurysm: A case report. J Clin Images Med Case Rep. 2023; 4(5): 2394.
Introduction
Delayed Cerebral Ischemia (DCI) is a frequent and serious complication after Subarachnoid Hemorrhage (SAH), the leading cause of disability and fatality in survivors of SAH, the most important complications of stent-assisted coil embolization of cerebral aneurysms, and one of the complications after clipping surgery of aneurysm. However it has been rarely reported after coil embolization of unruptured cerebral aneurysms without stent assistance. Here we reporta 72-year-old patient prensenting with DCI, which occurred 6 days after coil embolization for the treatment of a giant unruptured communicating segment aneurysm of internal carotid without stent assistance. The symptom of DCI showed rapid spontaneous remission with the National Institute of Health Scale Score (NIHSS) changing from 27 to 9. He recovered gradually to a score of 0 in NIHSS and the Magnetic Resonance Imaging (MRI) of the brain revealed watershed infarction after intravenous thrombolysis with rt-PA. The primary thrombosis embolism may be generated in the neiborhood of the giant aneurysm, and its pathophysiology is perhaps as follows: the incomplete occlusion influenced the local hemodynamic effectthat caused turbulence and the presence of thrombus. The thrombolysis was made partly because of its unstability and partly because of the effect of the drug. Both the compressive stenosis of the initial segment of bilateral Anterior Cerebral Arteries (ACA) and the hypovolemia followed diarrhea accelerated the fragment of thrombus to flow to the watershed.
Case report
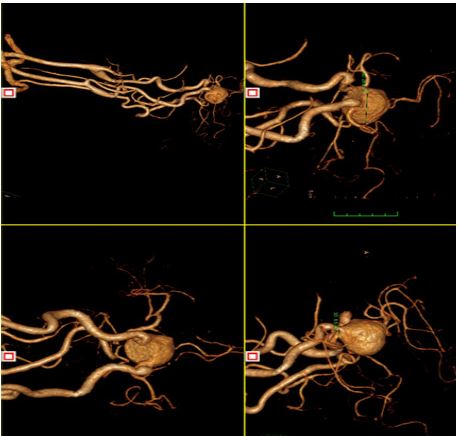
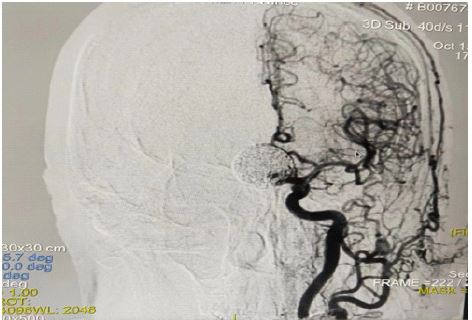
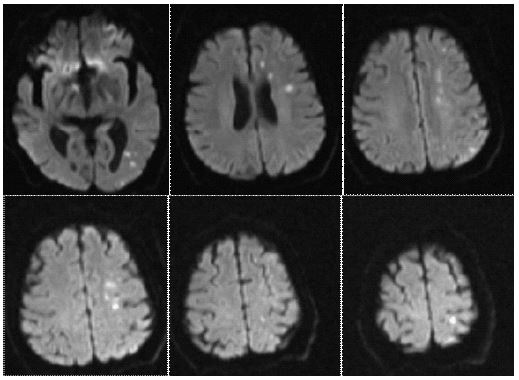
A 72-year -old man was admitted due to his being found in an unconscious state for 1 hour. He was normal 3 hours ago before his admission. He was lying on the sofa, showing no reaction to others voice. Neither seizures nor gaze of the double eyeballs was found. He vomited once during his being transported to the hospital and the color of the vomitus was brown. He had a history of hypertension for many years and was administered with 2.5 mg levoamlodipine once daily recently. He has agiant unruptured communicating segment aneurysm of internal carotid (Figure 1) and accepted endovascular coil embolization without stent assistance 6 days ago. The grade was III according to the Raymond-Roy classification (class I, complete obliteration; class, residual neck, and class III, residual aneurysm) (Figure 2) [1]. He suffered for acute diarrhea in the past 2 days. Physical examination on admission was as follows: T 36.7, P 64 bpm, R 16 bpm, BP 130/70 mmHg. He was in a sopor state. His pupils was in the normal size and reflexed sensitively to the light. He showed no neck resistance, negative Kernig sign, and negative Bruzinski sign. His left limbs showed involuntary movement while the right ones didn’t move at all. The National Institute of Health scale score (NIHSS) was 27. Color Doppler ultralsound of the heart and the cervical arteries was taken 10 days ago which showed a normal heart and there was no arterial stenosis. His electrocardiogram was normal. The preliminary diagnosis was made as follows: hemorrhagic stroke? ishchemic stroke? Epilepsy mimicking stroke ? CT scan of the brain showed no obvious abnormality. After the CT examination he recovered a lot with the NIHS slowed down to 9 gradually. After the occult blood testing of vomitus gave a negative result we gave the patient rt-PA intravenous thrombolysis (0.9 mg/kg) which result in an perfect clinial manifestation and the NIHSS became 0 the next day. Subsequently, the Magnetic Resonance Imaging (MRI) of the brain was perfomed and it revealed that there were acute cerebral infarction lesions in the watershed area (Figure 3). Magnetic Resonance Angiopathy (MRA) showed compressive stenosis in the initial segment of the bilateral Anterior Cerebral Arteries (ACA) (Figure 4). The patient was then treated with 100mg aspirin once daily, and was discharged 1 week later.

Discussion
Clipping surgery and endovascular coil embolization are two different methods for the treatment of cerebral aneurysms. It is still controversial about which is the best choice for treatment of unruptured cerebral aneurysms. Many researches show that coil embolization is of great advantage due to its low fatality and disability rate [2,3]. It was managed by coil embolization in this case. As for unruptured cerebral aneurysms, perforation occurs in 0.5-2.4% of the patients treated through endovascular method [4], both intra procedural rupture and delayed rupture are included [5,6]. Besides, remote intraparenchymal hemorrhage can also happens after end ovascular treatment [6]. Due to the symptoms of unconsciousness and vomitting which may indicate high intracranial pressure, delayed ruputure of the aneurysm, remote intraparenchymal hemorrhage and intraprocedural rupture which led to the advance of clinical features were first suspected. However CT imaging of the brain denied all of them. Then Acute Ischemic Stroke (AIS) was considered. But regretfully, we didn’t apply MRI immediately because there was risk of apnea caused by vomitting. In addition epilepsy which mimicked stroke couldn’t be excluded based on the mass effect of the giant aneurysm and unclear onset of clincial manifestations, while the improving consicousness and the neurolgical function defect which may indicate TODD paralysis could be the evidence of epilepsy. It was difficult to make an exact diagnosis at that time. In consequence of the idea that time is brain, considering the potential disability of AIS, intravenous thrombolysis with rt-PA (0.9 mg/kg) was exerted to him. Further improvement after thrombolysis supports the effectiveness of thrombolytic therapy for acute ischemic stroke on one hand, but does not rule out the natural outcome of todd paralysis after epileptic seizures on the other hand.
MRI was examined later. The compressive stenosis of the initial segment of the bilateral ACA showed by MRA provides the anatomical basis for cerebral infarction in the watershed area theoretically. And the diarrhea before the neurological deficit may cause hypovolemia and cerebral hypoperfusion which can be the pathophysiological basis of watershed cerebral infarction. However, AIS in the watershed does not explain the disturbance of consciousness. Therefore, we inferred that the cerebral infarction lesions in the watershed area are secondary changes after thrombus. The primary lesion should be locateing in the upstream artery. Combined with the coil embolization 6 days ago, we think it may be in the neiborhood of the giant aneurysm.
So what is the etiology of AIS in this case? According to the modified TOAST system [7], the most common etiology is atherosclerotic, followed by cardioembolism. However, neither the result of color Doppler ultrasound nor the imaging of DSA during the interventional procedure supports them. Therefore, we think its essential etiology is DCI. DCI was first described by Gull in 1859, based on the symptoms of neurological deficit in a patient with Subarachnoid Hemorrhage (SAH). Different literatures illustrate various definitions of DCI, the most appropriate one is suggested to be cerebral infarction by Mervyn et al. in 2011 [8]. It is a frequent and serious complication after SAH, the leading cause of disability and fatality in survivors of SAH [9,10], the most important complications of stent-assisted coil embolization of cerebral aneurysms [11], and one of the complications after clipping surgery of aneurysm [12,13]. However, it’s a relatively rare complication after coil embolization without stent assistance of unruptured cerebral aneurysms. ARETA, a prospective multicenter study in endovascular treatment for unruptured aneurysms, shows that all the DCI events happened in the weeks following the procedure [14]. In this case it occurred 6 days after treatment of endovascular coil embolization, which coincides with the aforementioned study. Since no stent was used to assist the coil embolization, what’s the pathophysiology of the DCI in this case? The aneurysm can be recanalized, grow, and rupture if it is incompletely occluded. Thus it’s a useful way to assess the risk of recurrence and reperforation for treated aneurysms by assessing the occlusion degree and their parent arteries [15].
However, there is still not enough attention on the DCI after incomplete occlusion nowadays. It was reported the incidence rate of DCI was 9.4% in patients with post-procedure aneurysm remnant while it‘s only 1.6% in those with adequate occlusion [14]. Raymond-Roy classification is widely used to assess the degree of aneurysm occlusion. We think that incomplete occlusion leads to the formation of a dead space, which in turn causes blood flow disturbance, stagnation, and eventually leads to the DCI event although no stent had been used during the interventional procedure. So the grade of Raymond-Roy classification may be helpful to estimate the possibility of DCI event. Advances in interventional embolization techniques and materials may be expected to improve the degree of embolization and reduce DCI in such patients.
DCI is a common complication in patients with SAH and aneurysm stent-assistedinterventional embolization. Prevention is more important than treatment in some scholars’ opinions [16]. Dual antiplatelet therapy has become the standard for prevention of these diseases, but it is still not standardized [17]. In the circumstances such as this case when the aneurysm was unruptured, and the stent-assisted technique was not employed during the endovascular treatment, it seems to be inappropriate for routine antiplatelet therapy unless there are other diseases that require antiplatelet therapy. It needs further research to clarify whether there would be potentially fatal complications such as thrombocytopenia and bleedings if dual anti platelet therapy is applied.
Conclusion
In conclusion, the occurrence of DCI in this case may be related to clinical, technical and anatomical reasons. it seems that we still have a long way to go in the identification, prevention and treatment of DCI after coil embolization of unruptured aneurysms especially when no stent is used.
References
- Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001; 32 : 1998-2004.
- Pierot L, Barbe C, Nguyen HA, et al. Intraoperative Complications of Endovascular Treatment of Intracranial Aneurysms with Coiling or Balloon-assisted Coiling in a Prospective Multicenter Cohort of 1088 Participants: Analysis of Recanalization After Endovascular Treatment Of Intracranial Aneurysm (ARETA) Study. Radiology. 2020, 295: 381-389.
- Pierot L, Barbe C, Herbreteau D, et al. Rebleeding and bleeding in the year following intracranial aneurysm coiling: analysis of a large prospective multicenter cohort of 1140 patients-Analysis of Recanalization after Endovascular Treatment of Intracranial Aneurysm (ARETA) Study. J NEUROINTERV SURG. 2020; 12 : 1219-1225.
- Fiehler J, Byrne JV. Factors affecting outcome after end ovascular treatment of intracranial aneurysms. CURR OPIN NEUROL. 2009; 22: 103-108.
- Kawabata S, Imamura H, Adachi H, et al. Risk factors for and outcomes of intraprocedural rupture during endovascular treatment of unruptured intracranial aneurysms. J NEUROINTERV SURG. 2018; 10: 362-366.
- Jee TK, Yeon JY, Kim KH, et al. Treatment Outcomes After Single-Device Flow Diversion for Large or Giant Aneurysms. WORLD NEUROSURG. 2021; 153: e36-345.
- Han SW, Kim SH, Lee JY, Chu CK, Yang JH, Shin HY, et al. A new subtype classifica- tion of is chemic stroke based on treatment and etiologic. Eur Neurol. 2007; 57: 96–102.
- Vergouwen MD. Vasospasm versus delayed cerebral is chemia as an outcome event in clinical trials and observational studies. NEUROCRIT CARE. 2011; 15: 308-311.
- Caricato A, Silva S. Delayed cerebral ischemia: is it time to change our practice? MINERVA ANESTESIOL. 2020; 86: 1266-1268.
- Cremers CH, Cos PC, van der Schaaf IC, et al. CT perfusion during delayed cerebral ischemia after subarachnoid hemorrhage: distinction between reversible ischemiaand ishcemia progressing to infarction. NEURORADIOLOGY, 2015; 57: 897- 902.
- Song J, Yeon JY, Kim JS, et al. Delayed thromboembolic events more than 30 days after self expandable intracranial stent-assisted embolization of unruptured intracranial aneurysms. CLINNEUROL NEUROSUR. 2015; 135: 73-78.
- Campe C, Neumann J, Sandalcioglu IE, et al. Vasospasm and delayed cerebral ischemia after uneventful clipping of an enraptured intracranial aneurysm - A case report. BMC Neurol. 2019; 19: 226.
- Goertz L, Krischek B, Reiner M, et al. Penumbral salvage by delayed clip reposition 19 hours after cerebral aneurysm clipping - induced ischemia results in neurologic restitution - correlation with indocyanine green videoangiography and FLOW 800 measurements. WORLD NEUROSURG. 2020; 138: 61-67.
- Pierot L, Barbe C, Herbreteau D, et al. Delayed thromboembolic events after coiling of unruptured intracranial aneurysms in a prospective cohort of 335 patients. J NEUROINTERV SURG. 2021; 13: 534-540.
- Etminan N, de Sousa DA, Tiseo C, et al. European Stroke Organisation (ESO) guidelines on management of unruptured intracranial aneurysms. EUR STROKE J. 2022; 7: V.
- Koenig HM, Chen J, Sleg EP. Delayed cerebral ischemia: Is prevention better than treatment? J NEUROSURG ANESTH. 2021; 33: 191-192.
- Cheddar EI Aouni M, Magro E, Abdelrady M, et al. Safety and efficacy of cangrelor among three antiplatelet regimens during stent- assisted endovascular treatment of unruptured intracranial aneurysm: A single - center retrospective study. Front Neurol. 2022; 13: 727026.