Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Tubulovillous adenoma of the bile duct under direct
cholangioscopy
John M Iskander1*; Rody Yoshinaka2; Victoria O’Connor1
1Division of Gastroenterology, Kaiser Permanente Los Angeles Medical Center, USA.
2Division of Surgical Oncology, Kaiser Permanente Baldwin Park Medical Center, USA.
*Corresponding Author : John M Iskander
Department of Gastroenterology, Kaiser Permanente Los Angeles Medical Center, USA.
Email: john.m.iskander@kp.org
Received : Apr 24, 2023
Accepted : May 23, 2023
Published : May 30, 2023
Archived : www.jcimcr.org
Copyright : © Iskander JM (2023).
Citation: Iskander JM, Yoshinaka R, Connor VO. Tubulovillous adenoma of the bile duct under direct cholangioscopy. J Clin Images Med Case Rep. 2023; 4(5): 2436.
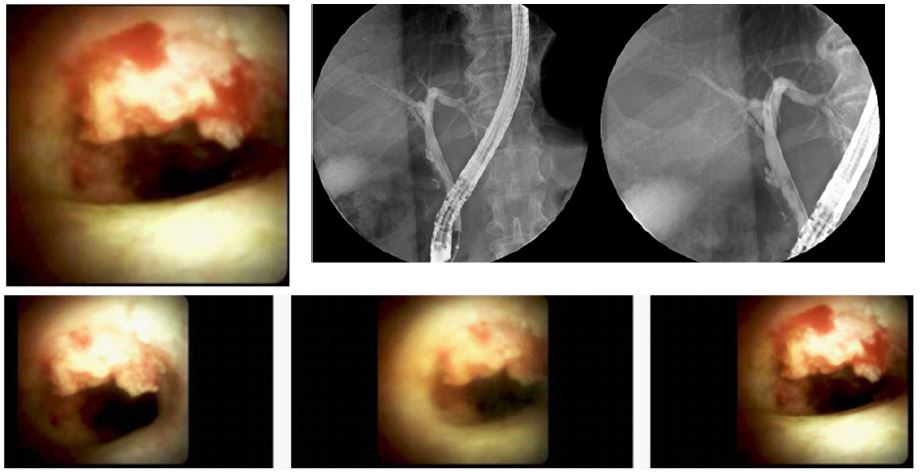
Description
A 56 year old male with chronic hepatitis B on entecavir therapy with a low viral load who underwent routine HCC screening with transabdominal ultrasound showing a dilated common bile duct. This was followed with MRCP which revealed choledocholithiasis. LFTs minimally elevated and only occasional right upper quadrant pain. Subsequently an ERCP was performed with stone extraction and incidentally extracted polypoid tissue showing tubulovillous adenoma histology. A biliary stent was placed at that time. A follow up EUS and ERCP with Spyglass DS (Boston Scientific, Marlborough, MA) directcholangioscopy was performed revealing a mid duct luminal nodule of nearly 15 mm size with directed forceps biopsies confirming persistent of a tubulovillous adenoma with high grade dysplasia. The patient was referred to surgical oncology and operative management ensued with a common bile duct resection, cholecystectomy and hepaticojejunostomy with final histology showing a 1.9 x 1.9 x 0.3 cm villous adenoma with high grade dysplasia and negative margins achieved (Tis N0 MX).