
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Oropharyngeal Kaposi’s sarcoma in a non-immunosuppressed patient
Encarnacion Navarro JA1,2*; De la Fuente Munoz MI1; Cardenas Canovas E1; Villanueva San Vicente V3;
Martinez Garcia J2,4; Velazquez F5; Alonso Romero Journal2,4; Garcia Fernandez R1; Quiles Hevia B1;
Romero Borque A1; Lopez Soler F1; Espinosa Lopez A1; Laborda Segovia A1; Lopez Jiménez E1; Manso Murcia C6
1Radiotherapy Oncology Department Virgen de la Arrixaca University Clinical Hospital, Murcia, Spain.
2Murcian Biosanitary Research Institute, Murcia, Spain.
3Department of Maxillofacial Surgery Virgen de la Arrixaca University Clinical Hospital, Murcia, Spain.
4Department of Medical Oncology Virgen de la Arrixaca University Clinical Hospital, Murcia, Spain.
5Department of Radiology, Virgen de la Arrixaca University Clinical Hospital, Murcia, Spain.
6Department of Intensive Care Medicine, Virgen de la Arrixaca University Clinical Hospital, Murcia, Spain.
*Corresponding Author : Encarnacion Navarro JA
Radiotherapy Oncology Department Virgen de la
Arrixaca University Clinical Hospital. Murcia, Spain.
Email: Juanan881@hotmail.es
Received : May 07, 2023
Accepted : Jun 02, 2023
Published : Jun 09, 2023
Archived : www.jcimcr.org
Copyright : © Navarro JAE (2023).
Abstract
Kaposi’s sarcoma is a malignant tumor caused by the HHV-8. It usually occurs in people with weakened immune systems, due to HIV/AIDS. We expose the diagnostic-therapeutic process of a 71-year-old man with an oropharyngeal Kaposi’s sarcoma due to infection with human herpes virus 8 without alteration of the immune system.
Keywords: Kaposi’s sarcoma; Kaposi’s sarcoma-associated herpes virus; Oropharyngeal neoplasms.
Citation: Navarro JAE, Munoz MIF, Canovas EC, San Vicente V, Garcia M, et al. Oropharyngeal Kaposi’s sarcoma in a non-immunosuppressed patient. J Clin Images Med Case Rep. 2023; 4(6): 2449.
Introduction
Kaposi’s sarcoma is a very rare entity in our environment but it can manifest as tumour lesions in multiple regions of the body. The most typical location is in the extremities and oral cavity, due to the high relationship with HIV, although this is not always the case, taking into account the underlying infection with HHV-8. The history, early detection and histology are pillars for treatment, where the patient’s profile, the aggressiveness of the tumour of the specific markers and the comorbidities mark the treatment to be followed. The clinic can be mixed, which makes us take into account the possible differential diagnoses. The fundamental pillars in treatment are surgery and radiotherapy, with excellent response rates, achieving local control and cure.
Clinical case presentation
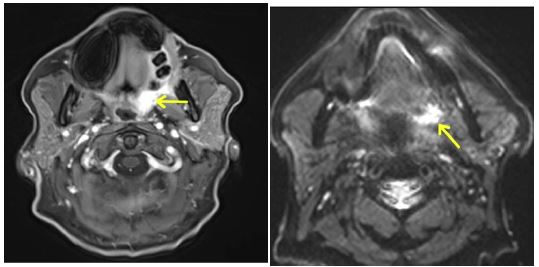
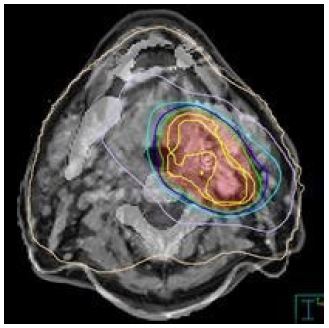
A 71-year-old male, diabetic in treatment with oral antidiabetics, with no other diseases of interest or toxic habits, who attended Maxillofacial Surgery Outpatient Consultations referred from Hecla for an ulcerated lesion in the left buccal mucosa of more than a year of evolution together with intermittent bleeding. In consultation, a tumour-like and hyperactive vascularized lesion was evidenced in the left oropharynx, requiring embolization prior to biopsy of the ascending palatine artery and small masseteric/buccal left branches, with success. After that, a Core Needle Biopsy (CNB) of the oropharyngeal tumour was performed, without complications, and it was sent to Pathology for an immunohistochemically study. In it, it was described as a proliferative vascular lesion, with apoptosis, without signs of mitosis, CD34+, CD31+, Valentin+, ERG+ and an intense and diffuse nuclear positivity for Human Herpes Virus 8 (HHV-8), all of which is suggestive of sarcoma of the Oropharyngeal Kaposi. Given this diagnosis, a clinical study was carried out with blood tests and serologist for HIV, which were negative and an extension radiological study was carried out with contrast with thoracic-abdominal-pelvic CT (TAP CT), cervical CT and crevice-mandibular MRI (Figure 1). After commenting on the case in the hospital’s Multidisciplinary Committee for Head and Neck Tumours, it was jointly decided to dismiss surgery for the time being due to extensive injury and to propose the option of radio chemotherapy (RTCT) with a radical attitude. Days later, he was assessed in Medical Oncology, where TAP CT was reported without significant lesions and a hyper-uptake lesion cantered on the left oropharyngeal wall with extension to the left soft hemi palate and retro molar trigone on CT and crevice-mandibular MRI. On examination, no pathological signs were found in the revision by apparatus and systems, except for a small single adenopathy in the left cervical chain, suggestive of reactivity, together with a stable juggle lesion and without active bleeding. With these data, it was sub classified as locally advanced left oropharyngeal Kaposi’s sarcoma in an HIV-negative patient, and radical curative treatment with subsequent Radiotherapy (RT) + Chemotherapy (CT) was proposed. He was referred to the Radiotherapy Oncology clinic to start treatment with external RT with the technique of Volumetric Intensity Modulated Arc Therapy (VMAT), with curative intent, up to a total dose of 44 Gy in 22 fractions (2 Gy/fraction), which requires a Simulation CT in the service to delimit treatment volumes (Figure 2). During treatment with RT, the patient developed grade 1 oropharyngeal pain and microsites, controlled with first-step analgesia, without dysphagia or other adverse effects, and was jointly supervised by the Nutrition section to assess possible nutritional deficits derived from fibrosis and treatment of the oropharyngeal area. At the end of the 22 sessions of RT, a spectacular improvement was observed from the initial symptoms. In the examination at the end of treatment, a complete resolution of the ulcerated area was evidenced together with closure of the edges of the affected buccal mucosa and visualization of a whitish fibrous plaque in its place (Figure 3). After completing RT, he began sequential CT with PEGylated liposomal doxorubicin at 20 mg/m2 every 14 days, completing 8 sessions and undergoing joint reviews by both. After 3 months, MRI and PET CT were performed, showing complete response.

Discussion
Classic Kaposi’s sarcoma is a neoplasm characterized by abnormal angiogenesis requiring human herpes virus 8 (HHV-8) infection, along with other cofactors, manifesting primarily as multiple vascular nodules in the skin and other organs. It most commonly arises in older adult men of Mediterranean and Central/Eastern European descent, but can also occur in younger people, women, and other geographic areas. The most common presentation is purple, reddish-blue, or dark brown/black skin lesions (macules, nodules, plaques) on the lower extremities, often with lymphedema. The disease was first described by Kaposi as an idiopathic multiple pigmented sarcoma [1]. After Kaposi’s description, sporadic cases were reported. Interest resurfaced with the discovery of Kaposi’s sarcoma in a geographic belt in Africa and with the recent epidemic associated with Acquired Immune Deficiency Syndrome [2]. There are three forms of Kaposi’s sarcoma with differences between them: Classic form, endemic form (African) and epidemic (associated with AIDS). The classic form began in the early 20th century; it was observed that the disease was more common in southern and Eastern Europe than in northern and Western Europe, some studies showed that the disease is more frequent in Jews and in people of Mediterranean descent. This hypothesis is debatable. The highest incidence is observed in the fifth, sixth and seventh decades. Kaposi originally described multiple dermal plaques, nodules, and tumours. These are red or purplish in fair-skinned people, and darker than the surrounding skin, with a bluish tint, in dark-skinned people. As the lesions age or involute, they take on a brownish colour. The lesions begin as small papules and may progress to plaques, nodules, or tumours; they can reach 10 cm. in diameter or more and vary from one to one hundred, in a given patient. Tumours and nodules may be covered by normal, atrophic or ulcerated skin; some have a warty or fungal surface. Lesions are more common in the lower extremities and spread centripetally slowly. The lesions can burn, sting or hurt, in those located in the lower limbs the pain can limit walking. Enema is common, especially in the legs, and may be severe enough to limit walking. Spontaneous bleeding or bleeding secondary to trauma may occur. Any internal organ may be affected. The disease may be exclusively visceral without skin lesions. Death may result from generalized disease with cachexia, haemorrhage, or impaired function of vital organs due to tumour growth. The endemic form (African). In 1963 Lathe described an endemic belt in tropical Africa, including Kenya, Tanzania, and Zaire, where the disease is surprisingly common, constituting up to 9% of all malignant tumours, with a peak in the first decade of life [2]. Life, no cases are seen in the second decade, and then increases steadily throughout adult life. Endemic cases of Kaposi’s sarcoma present with a morphological diversity of lesions, which can be sub classified into four main types: Nodular, florid, infiltrative, and lymphadenopathy. This morphological classification has served to clinically identify distinct groups with different histological pictures, natural history and response to treatment. The nodular type is the most common and can coexist with other more aggressive tumours; it is indolent, with a variable response to treatment and can spontaneously recede. The florid variety is usually fast growing, ulcerated, with secondary infection, and haemorrhagic; these tumours can extend deep into the dermis and affect the bone, they respond dramatically to chemotherapy. The infiltrative type is usually limited to the hand or foot and is characterized by a deeply invasive, fibrotic, indurated tumour with a fleshy, nonbiting enema; Invasion and destruction of the underlying bone most commonly occur, these lesions are long-lasting and respond slowly, if at all, to chemotherapy. The lymphadenopathy type is more common in children and young adults and can be clinically confused with lymphoma. Skin nodules may or may not occur, the affected lymph nodes grow rapidly, and until recently, this form of Kaposi’s sarcoma had a poor prognosis. Aggressive use of chemotherapy can produce rapid regression with some long-term survivors.
The form associated with AIDS. The AIDS epidemic, which in mid-1983 comprised more than 1,500 cases, was originally heralded by a high number of cases of Kaposi’s sarcoma and Pneumocystis carina pneumonia in homosexual men. The association of Kaposi’s sarcoma and AIDS was based on severe functional immunodeficiency, similar to the situation observed in immunosuppressed allograft recipients. The clinical characteristics and the evolution of the disease in patients with AIDS differ from the endemic and classic forms [3]. Kaposi’s sarcoma in immunosuppressed patients begins as a reddish macule with perilesional paleness. Within a week, the macula changes to a purple or brown colour and the pale halo disappears. The tumours are small, just a few millimetres to a centimetre, round, slightly raised, and grow slowly over weeks or months. Rarely, a single skin tumour occurs, frequently on the sole of the foot, or on the head and cervical region, but most patients present with multiple lesions widely distributed throughout the body; occasionally some patients develop a mirror-symmetric distribution. Approximately 10% of patients present with peripheral lymph node involvement as a manifestation of Kaposi’s sarcoma; in these cases, the tumour is of sub capsular or trabecular location. 50% of patients develop lesions in the mouth or in the gastrointestinal tract; they are located in the submucosa and are purple-red in colour. In deceased patients with advanced skin disease, Kaposi’s sarcoma is found in virtually all organs except the brain. The natural history of untreated disease in AIDS patients is variable. A minority presenting with one or two skin lesions remain stable for a few years. The lesions usually grow slowly and new tumours appear within weeks to months.
Oral cavity
Oral cavity involvement occurs in approximately one-third of KS patients and is the initial site in approximately 15 percent. The most commonly affected intraoral site is the palate followed by the gingiva. Intraoral lesions can be easily traumatized during normal chewing, which can lead to pain, bleeding, ulceration, or secondary infection. If the lesions are advanced, they can interfere with nutrition and speech. The presence or absence of symptoms of oral lesions is often an important factor in treatment decisions [4].
Treatment
There is no consensus on the optimal tumour-directed therapy for the different classic manifestations of KS. Because many active treatments have been described, therapeutic choices are often made based on the experience and medical discipline of the treating physician, but also include consideration of patient preferences and comorbid conditions. For patients who have volume-limited disease causing symptoms (eg, bleeding or chafing on clothing) or cosmetic disfigurement, we suggest local treatment rather than observation or systemic chemotherapy. The choice of modality (radiotherapy, excision, cryotherapy, laser ablation, intraregional, or topical therapy) depends on several factors, including the site and extent of disease, as well as physician and patient preference. For patients with an indication for chemotherapy and without cardiac contraindications, we suggest PEGylated liposomal doxorubicin as initial therapy over other available agents. All forms of Kaposi’s sarcoma, including classic, are highly sensitive to RT. However, due to the multifocal nature of the disease, the persistence of HHV-8 even with successful local control of the lesion, and the tendency for new lesions to develop in non-irradiated areas, there is no consensus on the place of RT. in the therapeutic arsenal. There is marked variation in total RT doses (6 to 60 Gy) and fractionation regimens, ranging from doses of 6 to 12 Gy in a single fraction to larger total doses given in smaller fractions over several weeks [5-7]. One of the most commonly prescribed regimens is 30 Gy in 15 daily 2-Gy fractions [8,9].
References
- Kaposi M. Idiopathisches multiples pigmentsarkom der Haut Arch Derm Syph. 1872; 4: 265.
- Lothe F. Kaposi’s sarcoma in Uganda africans. Acta Pathol Microbiol Scand. 1963; 161: 5.
- Friedman-Kien AE. Disseminated Kaposi’s sarcoma in homosexual men. Ann Intern Med. 1982; 96: 693.
- Nichols CM, Flaitz CM, Hicks MJ. Treating Kaposi’s lesions in the HIV-infected patient. J Am Dent Assoc. 1993; 124: 78.
- Huang KM, Hsu CH, Cheng JC, Lai MK, Jeng SC, et al. Radiotherapy of classic Kaposi’s sarcoma in Taiwan, an area where classic Kaposi’s sarcoma is not prevalent. Anticancer Res. 2006; 26: 4659.
- Chang LF, Reddy S, Shidnia H. Comparison of radiation therapy of classic and epidemic Kaposi’s sarcoma. Am J Clin Oncol. 1992;15: 200.
- Caccialanza M, Marca S, Piccinno R, Eulisse G. Radiotherapy of classic and human immunodeficiency virus-related Kaposi’s sarcoma: results in 1482 lesions. J Eur Acad Dermatol Venereol. 2008; 22: 297.
- Hauerstock D, Gerstein W, Vuong T. Results of radiation therapy for treatment of classic Kaposi sarcoma. J Cutan Med Surg. 2009; 13: 18.
- Kirova YM, Belembaogo E, Frikha H, Hadded E, Calitchi E, et al. Radiotherapy in the management of epidemic Kaposi’s sarcoma: a retrospective study of 643 cases. Radiother Oncol. 1998; 46: 19.