
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Ovarian tuberculosis: Challenges in diagnosis in a low resource settings
Yahya Magaso1; Dismas Matovelo1*; Leonard Washington3; Richard Kiritta1; Edrick Elias2; Oscar Ottoman2; Godfrey Kaizilege1; Edgar Ndaboine1
1Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied sciences, Mwanza, Tanzania.
2Department of Pathology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Mwanza, Tanzania.
3Department of Surgery, Bugando Medical Centre, Catholic University of Health and Allied sciences, Mwanza, Tanzania.
*Corresponding Author : Dismas Matovelo
Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied sciences, Mwanza, Tanzania.
Email: magonza@bugando.ac.tz
Received : Jun 09, 2023
Accepted : Jun 27, 2023
Published : Jul 04, 2023
Archived : www.jcimcr.org
Copyright : © Matovelo D (2023).
Abstract
Background: Tuberculosis continues to be endemic in developing countries. Despite genitourinary tuberculosis being common, reports of isolated ovarian tuberculosis are rare, further its presentation can mimic that of ovarian cancer. Challenge arises when evaluating patients who lack usual clinical symptoms and laboratory evidence required for correct diagnosis.
Case Presentation: A 19-year-old female presented to our facility with a history of undergoing exploratory laparotomy 3-months prior at rural district hospital due to a pelvic mass and no biopsy was taken. Laboratory examination revealed an increase in cancer antigen (CA-125) and normal serum beta-Human Chorionic Gonadotropin (HCG) and Alpha Fetal Protein (AFP) levels. Both pelvic ultrasound and Magnetic Resonance Imaging (MRI) yielded inconclusive results. As a result, the decision for re-laparotomy was made due to presumptive diagnosis of ovarian tumor. Surgical excision of a solid ovarian mass was done during surgery and histopathological examination later revealed presence of ovarian tuberculosis. Thereafter, anti-TB drugs were started and worked well, as shown by the disappearance of symptoms, and the return of CA 125 levels to normal.
Conclusion: High index of suspicion is needed by clinicians dealing with cases of ovarian mass with atypical clinical, laboratory and radiological findings and should weigh the benefits of ultrasound-guided biopsy against risks of invasive surgery.
Keywords: Ovarian tuberculosis; Ovarian Cancer; Chronic pelvic pain; Laparotomy.
Abbreviations: AFP: Alpha- Feto Protein; ADA: Adenosine Deaminase; BMC: Bugando Medical Centre; BP: Blood Pressure; CA: Cancer Antigen; EPTB: Extrapulmonary Tuberculosis; HCG: Human Chorionic Gonadotropin; MRI: Magnetic Resonance Imaging; PTB: Pulmonary Tuberculosis; TB: Tuberculosis; WHO: World Health Organization.
Citation: Magaso Y, Matovelo D, Washington L, Kiritta R, Elias E, et al. Ovarian tuberculosis: Challenges in diagnosis in a low resource settings. J Clin Images Med Case Rep. 2023; 4(7): 2483.
Background
Tuberculosis is a chronic granulomatous disease caused by Mycobacterium Tuberculosis [1]. It mainly affect the lungs causing Pulmonary Tuberculosis (PTB), however tubercle bacilli can spread to other parts of the body causing Extrapulmonary Tuberculosis (EPTB) which accounts for 19.3% of all notifiable TB cases, it is estimated that Genital Tuberculosis (GTB) affects about 12% of women with PTB and 15-20% of women with EPTB [2,3]. The commonest site of involvement of GTB are the fallopian tubes in 90-100% and the endometrium in 50-80% of the cases, while the isolated ovarian tuberculosis occurs in 20-30% of cases of genital tuberculosis [4]. Globally, tuberculosis incidence rates have been on the decline for over 2-decades [5]. However, the rate of EPTB has not been decreasing in Low-Middle Income Countries (LMICs) [6]. Globally, approximately 10.0 million people developed TB disease in 2019 and an estimated 1.2million TB deaths [7].
EPTB cases usually have atypical presentation making diagnosis and identification delayed, and requires special clinical alertness to recognize the condition [6]. This case presents diagnostic challenges of ovarian tuberculosis at Bugando Medical Centre (BMC), Mwanza, Tanzania.
Case presentation
A 19-year-old woman Sukuma in tribe reported to our facility on November 15, 2021 with complaints of recurrent abdominal mass three months post-laparotomy, weight loss, constipation, and chronic pelvic pain. She had mass removed at a district hospital in which no histological evaluation was done. She had menarche at 13-years and was not sexually active. She had no neither TB contact, nor any TB symptoms.
She was stable, conscious, but emaciated. Her blood pressure was 110/70 mmHg, pulse rate 84 b/min, respiratory rate 16 cycles/min, body temperature 36.8oC, and oxygen saturation 99% in room air. Her respiratory, cardiovascular, musculoskeletal, and nervous systems were normal. The abdomen was moderately distended with a vertical sub-umbilical incision scar, no ascites and a palpable 6 x 5 cm pelvic mass on the left iliac and lumbar regions.
Her abdominal-pelvic ultrasound revealed a left adnexa mass with unknown origin. Due to inconclusive ultrasound results, MRI was recommended, which showed a 7 x 5 x 4 cm right adnexa mass. The mass’s nature and origin were unknown. Tumor markers: HCG= 1.80 mlU/ml (5.0 mlU/ml), and AFP= 0.5 ug/L (0.2-8.5 Ug/l), but CA-125= 135 ng/dl. Raised CA-125 and pelvic mass suggested ovarian tumor.
Due to inconclusive tumor markers and imaging reports, re-laparotomy was performed to complete cytoreduction. The right ovary was intact, but the right fimbria end was adhered to the mass, revealing massive abdominal adhesions. The left ovary and left tube were not appreciated because the mass occupied the left adnexa region from the sigmoid colon to the posterior bladder wall (Figure 1).
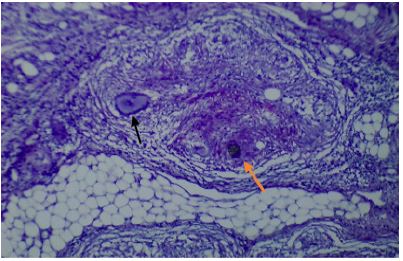
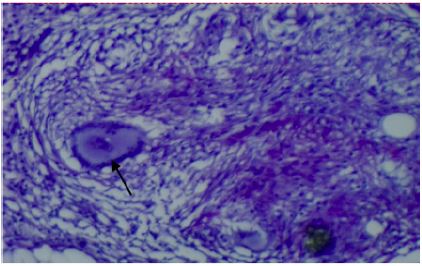
The uterus was normal, but part of the sigmoid colon, rectum, and posterior sigmoid colon were entrapped by the mass, causing luminal compression/obstruction. A 250 ml foul-smelling pelvic abscess was drained. Enterolysis, adhesiolysis, and 50% mass excision was achieved. Abdomen was irrigated with warm saline. Just proximal to the rectosigmoid junction, an end loop colostomy was performed. She had a smooth post-operative period and went home after 5 days. Histology results revealed features of chronic granulomatous inflammation with caseous necrosis consistent with ovarian tuberculosis (Figure 2 & Figure 3).

Aura mine, ZN stain, and chest X-ray testing were all negative. She began anti-TB therapy 2-months after surgery and eventually, the colostomy was closed on August 17, 2022. A CT scan showed no abdominal mass after six months of anti-TB treatment. Her weight increased from 44.2 kg prior to anti-TB to 59.5 kg end of anti-TB therapy. On 17th August 2022: bBarium enema and abdominal pelvic CT scan indicated no abdominopelvic mass in which colostomy closure was done.
Discussion
Tuberculosis is a chronic granulomatous disease caused by Mycobacterium Tuberculosis [1]. It is a disease with 95% of deaths occurring in the developing world [8]. It typically affects the lungs, causing Pulmonary Tuberculosis (PTB), although tubercle bacilli can infect other body organs, causing Extrapulmonary Tuberculosis (EPTB) [2]. In 15-25% of pelvic tuberculosis cases, ovarian tuberculosis originates from fallopian tube extension [4].
Globally, tuberculosis incidence rates have been on decline for over 2-decades [5]. However, the rate of EPTB has not been decreasing in LMICs due to a slow progress in TB care and prevention [6]. Globally, an estimated 10.0 million people developed TB in 2019, and there were an estimated 1.2 million TB deaths among HIV- negative people [9]. Ovarian TB like several other EPTB cases has atypical presentation leading to delayed diagnosis, needing clinical alertness to diagnose [6]. Our patient had two major surgeries, in which TB wasn’t detected leading to delayed treatment until histology reports. This delay in detection and treatment could have led to further consequences, even death.
More than 90% of TB patients live in LMICs [10]; where the diagnosis of TB rely primarily on the identification of acid-fast bacilli on sputum smears by conventional light microscope [11]. The sputum smear microscopy is relatively simple, inexpensive and highly specific for Mycobacterium tuberculosis in TB-endemic countries [12]. This requires serial smear sputum specimen, although it has 80% sensitivity compared to culture is some settings [13]. However, in other reports its sensitivity had been ranging between 20-80% [11].
TB smear microscopy is usually followed by culture for confirmation, because acid-fast bacilli visualized on a slide may represent Mycobacterium tuberculosis or non-tuberculous mycobacteria, so species identification and drug susceptibility test requires culture [14]. However, Mycobacterium tuberculosis culture is more feasible in developed countries due to its extended incubation period, being expensive than smears, and requiring specialized equipment [15]. Unfortunately, similar to other LMIC settings we have very few reference laboratories capable of reliably performing TB culture and Drug Susceptibility Test (DST) [11].
In this case, ZN staining was negative even after auramine test as special staining [16]. Again, despite use of LED microscopy, the test still remained negative for TB. World Health Organization (WHO) has been recommending ZN staining for the diagnosis of TB. It is advised that the conventional fluorescence microscopy be replaced by LED microscopy in all settings where fluorescent microscopy is now used and that LED microscopy be an alternative for conversional ZN stain in both high and low volume laboratories [17].
Despite the patient had no TB-contact, TB should be suspected in patients with (cough greater than 2-3 weeks, lymphadenopathy, fevers, night sweats, weight loss) and relevant epidemiological factors such as history of prior TB infection or past/-present history of travel to TB endemic area [18]. In our patient, the only features were weight loss, pelvic mass, and constipation, which can be present in other chronic conditions thus making TB diagnosis unlikely.
Tanzania is among countries with the highest burden of TB in the world [19]. According to WHO, 142,000 people fell ill with TB in 2018, of whom 40,000 (28%) were people living with HIV. However, only 75,828 people with TB were notified, leaving 47% of people still unreached by the national TB services [19].
In endemic regions, Adenosine Deaminase (ADA) can play a great role in the diagnosis. It is a polymorphic enzyme involved in the purine metabolism, catalyzes the deamination of adenosine to inosine and ammonium [20]. Although ADA is found in many tissue, it is numerous in lymphoid tissues mainly T-lymphocytes [20,21]. Our patient, ADA level was not done since she had no clinical features suggestive of TB pleurisy and this should be supported by chest x-ray findings, hence no thoracentesis was performed [22]. The ADA activity useful in TB diagnosis ranges from 40 to 70 U/L, the best results are yielded at 50U/L which corresponds to a sensitivity and specificity of 90% and 89% respectively [7,23].
Also, our patient, CA-125 was elevated about four folds, this increased more suspicious of advanced ovarian tumor. This is a protein which is produced by ovarian surface epithelium, used for ovarian cancer surveillance and monitoring of chemotherapy response [24]. However, the CA-125 lack specificity for ovarian cancer since it can rise in other conditions including malignancy, inflammatory processes, benign chronic conditions [25]. The rise of CA-125 in our patient was likely due to peritoneal inflammation by TB which has been seen in similar cases from other settings [16,26,27].
In this case, both ultrasound and MRI gave inconclusive results. Imaging has shown to have low specificity, with both ovarian malignancy and tuberculous abscess due to both pathologies having similar appearances on ultrasound, CT scan and MRI [28]. However, one study recommended ultrasound guided biopsies preoperatively [27]. Studies have shown laparoscopy to have a great advantage as it allows the diagnosis of TB in more than 97% of cases whilst avoiding laparotomy [28,29]. Laparoscopy was not performed due to lack of equipment skilled personnel and necessary surgical equipment [16].
In low-resource settings, ovarian tuberculosis can mimic ovarian cancer. In most cases, ovarian tuberculosis presents with no typical symptoms, with only elevated CA-125. Clinicians should have a high index of suspicion for ovarian tumors with unusual clinical and laboratory findings and should weigh the benefits of ultrasound-guided biopsy against the risks of invasive surgery.
Conclusion
All surgically removed masses should be subjected to histopathological examination. In TB-endemic regions, TB workup should be done concurrently before invasive surgery to avoid delay in diagnosis and treatment.
Declarations
Ethics approval and consent to participate: Not applicable
Consent for publication: Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Availability of data and materials: Not applicable
Competing interests: The authors declare that they have no financial and non-financial competing interests.
Funding: The cost of care to this patient was waived by the patient herself and her relatives as per hospital protocol. The cost of preparing the manuscript and publication was covered by the authors and Directorate of research and publications-Catholic University of Health and Allied Sciences.
Authors’ contribution: YM and DM played equally in evaluating the patient before surgery, follow-up during medical management and initial drafts of the manuscript. EN, LW, and GK played equal roles in evaluating the patient before surgery, performed surgery. EE and OO did histopathological studies of samples. RK followed the patient post-surgery. All authors read and approved the final version of the manuscript.
Acknowledgment: We are grateful to all clinical departments at BMC for the surgical interventions, timely interpretation of tissue biopsy sent for histological evaluation and medical management given thereafter.
Patient perspective: The care provided to the patient was timely with a follow up plan.
Timeline: The patient was first seen at our clinic on November 15, 2021, operated on November 25, 2021, and started anti-TB in February 2022. She has completed six months of anti-TB treatment and is cured. The colostomy was closed on August 17, 2022, and on August 29, 2022, which is twelve days post colostomy closure, she was seen at surgical outpatient department for post-op follow-up. She has improved, for she is passing stool per anus, there is no abdominal distension or vomiting, she is having no fever and there is no blood in stool.
References
- Brandli O. The clinical presentation of tuberculosis. Respiration. 1998; (65): 97–-105.
- Kulchavenya E. Extrapulmonary tuberculosis: Are statistical reports accurate?. Ther Adv Infect Dis. 2014; 2(2): 61–-70.
- Gatong DK, Gitau G, Kay V, Ngwenya S, Lafong C, Hasan Aet al. Female genital tuberculosis. Obs Gynecol. 2005; 7(2): 75–-79.
- Sharma JB. Current diagnosis and management of female genital tuberculosis. J Obs Gynaecol India. 2nd ed. 2015; 65(6): 362–-371.
- Glaziou P, Floyd K, Raviglione MC. Global epidemiology of tuberculosis. In Seminars in respiratory and critical care medicine. 2018 Jun; (Vol. 39, No. 03,: pp. 271-285).
- Ben Ayed H, Koubaa M, Marrakchi C, Rekik K, Hammami F, Smaoui Fet al. Extrapulmonary tuberculosis: Update on the epidemiology, risk factors and prevention strategies. Int J Trop Dis. 2018; 1(006).
- Piras M, Gakis C, Budroni M, Andreoni G. Adenosine deaminase activity in pleural effusions: aAn aid to differential diagnosis. BMJ. 1975;( 3): 192–-193.
- World Health Organization. Global Tuberculosis Report. 2013.
- Chakaya J, Khan M, Ntoumi F, Aklillu E, Fatima R, Mwaba P et al. Global Tuberculosis Report 2020: Reflection on the Global TB burden,treatment and Prevention efforts. Int J Infenctious Dis. 2021; 113(1): S7–-12.
- Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC. Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence and death globally. JAMA. 2005; 293(22): 2767–-2775.
- Steingart KR, Ramsay A, Pai M. Optimizing sputum smear microscopy for dignosis of Pulmonary tuberculosis. Expert RevAnti Infect. 2007; 5(3): 327–-331.
- Luelmo F. What is the role of sputum microscopy in patients attending health facilities? In: Toman’s tuberculosis: Case Detection,Treatment, and Monitoring-Questions and Answers. Frieden TR (Ed.). 2004;. 7–-10 p..
- Behr MA, Warren SA, Salamon H, Hopewell PC, De Leon AP, Daley CL et al. Mycobacterium tuberculosis from patients’ smear -negative for acid -fast bacilli. Lancet. 1999; 353(9151): 444–-449.
- Prince DS, Peterson DD, Steiner RM, Gottlieb JE, Scott R, Israel HL et al. Infenction with Mycobacterium avium complex in patients without predisposing conditions. N Engl J Med. 1989; 321(13): 863.
- Evans CA. Gene Xpert-a game -Changer for Tuberculosis Control? PLoS Med. 2011; 8(7).
- Kiritta R, Mrisho F, Mbulwa C, Miltenburg AS, Kihunrwa A. Extensive surgery for peritoneal tuberculosis, an on going diagnostic challenge in resource limited setup. JCIMCR. 2021; 2(2): 1093.
- World Health Organization. Report of the 9th meeting of STAG-TB, Geneva, Switzerland. 2009.
- Lewinsohn DM, Leonard MK, LoBue PA, Cohn DL, Daley CL, Desmond E et al. Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. 2017; 64(2).
- WHO. United Republic of Tanzania-TB Community Network: Aa platform for a stronger community response to tuberculosis. 2020.
- Van der Weyden MB, Kelley WN. Human adenosine deaminase distribution and properties. Biol Chem. 1976; (251): 5448–-5456.
- Randall W, Barton IG. Nucleotide metabolizing enzymes and lymphocytic differentiation. Mol cell Biochem. 1979; (28): 135–-147.
- Burgess LJ, Maritz FJ, Le Roux I, Taljaard JJ. Use of adenosine deaminase as a diagnostic tool for tuberculous pleurisy. Thorax. 1995; (50): 674–-676.
- Valdés L, San José E, Alvarez D, Sarandeses A, Pose A, Chomón B et al. Diagnosis of tuberculous pleurisy using the biologic parameters adenosine deaminase, lysozyme and interferon gamma. Chest. 1993; (103): 458–-465.
- Pepin K, Carmen M, Brown A, Dizon DS. CA 125 and epithelial ovarian cancer: Role in screening, diagnosis, and surveillance. Am J Hematol Oncol. 2014;( 10).
- Straughn JM, Robertson MW, Partridge EE. A patient presenting with a pelvic mass, elevated ca-125, and fever. Gynecol Oncol. 2000; (77): 471–-472.
- Chien JC, Fang CL, Chan WP. Peritoneal tuberculosis with elevated CA -125 mimicking ovarian cancer with carcinomatosis peritonei: Crucial CT findings. EXCLI journal. 2016; (15): 711.
- Wu CH, Changchien CC, Tseng CW, Chang HY, Ou YC LH. Disseminated peritoneal tuberculosis simulating advanced ovarian cancer: A retrospective study of 17 cases. Taiwan J Obstet Gynaecol. 2011;( 50): 292-296.
- Nebhani M, Boumzgou K, Brams S, Laghzaoui M, El Attar H, Bouhya S, et al. Pelvic tuberculosis mimicking bilateral ovarian tumor, A case report. Obs Gynecol Reprod Biol. 2004; 33(2): 145-147.
- Capsi B, Wolach V, Von Der Walde J, Weiss Y, Appelman Z, Hagay Zet al. Diagnosis of abdominal tuberculosis by transabdominal ultrasound guided needle biopsy. Ultrasound Obs Gynecol. 2000; 16(6): 569–-570.