
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
FDG-avid omental cake from ovarian cancer
Yassir Benameur*; Omar Ait Sahel; Salah Nabih Oueriagli; Abderrahim Doudouh
Department of Nuclear Medicine, Mohammed V Military Teaching Hospital, Rabat, Morocco.
Faculty of Medicine and Pharmacy, Cadi Ayyad University, Marrakech, Morocco.
*Corresponding Author : Yassir Benameur
Department of Nuclear Medicine, Mohammed V Military Teaching Hospital, Mohammed V University of Rabat, Morocco.
Tel: +212661209162 & +212537852406;
Email: benameur.yassir@gmail.com
Received : Jun 27, 2023
Accepted : Jul 11, 2023
Published : Jul 18, 2023
Archived : www.jcimcr.org
Copyright : © Benameur Y (2023).
Keywords: FDG; PET/CT; Ovarian cancer; Peritoneal carcinomatosis.
Citation: Benameur Y, Sahel OA, Oueriagli SN, Doudouh A. FDG-avid omental cake from ovarian cancer. J Clin Images Med Case Rep. 2023; 4(7): 2504.
Description
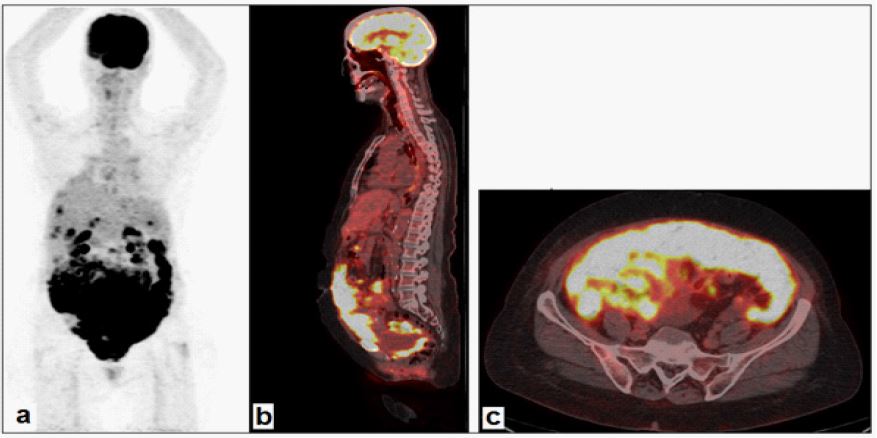
A 65-year-old multiparous patient presented to our hospital with vague abdominal pain for 2 months. Physical examination revealed normal bowel sounds in all four quadrants, with a soft and non-tender abdomen. Distension and dullness in percussion were noted. Initial investigations with abdominal Ultrasound (US) and Computerized Tomography (CT) revealed peritoneal fluid, and evaluation of the peritoneal fluid showed an elevated white blood cell count while fulfilling criteria for exudate. Serum tumor markers were elevated, suggesting an underlying malignancy. Apart from abdominal distension, the patient had no other gynecological complaints, and she declined any surgery. A whole body 18F-FDG-PET scan done 60 min after the intravenous injection of 300MBq of 18F-FDG demonstrated an unusually broad and prominent FDG-avid abdominal band in the region of the inferior abdomen and bilateral pelvic omental regions, and multiple nodular masses at the omentum with increased metabolic activity taking a pattern of FDG avid omental cake. An exploratory laparoscopy confirmed diffuse carcinomatosis in the omentum and the coloparietal region bilaterally, as well as surrounding small bowel loops, the transverse and sigmoid colon, and the rectum. The peritoneal biopsy proved this to be due to metastatic deposits of high-grade serous ovarian carcinoma.
This case illustrates an extraordinary presentation of metastatic ovarian cancer with massive peritoneal carcinomatosis visualized on FDG-PET/CT and an unusual aspect of “FDG-avid omental cake”. This term is used to describe serious and diffuse peritoneal carcinomatosis with a mass-like feature; metastatic disease is the most common cause of peritoneal metastasis and is usually associated with a poor prognosis [1]. The most frequent secondary cause of diffuse peritoneal infiltration is intraperitoneal tumor dissemination, which typically leads to ovarian, colorectal, and gastric cancers [2]. Inflammatory diseases such as tuberculosis, Crohn’s disease, phlegmonous pancreatitis, granulomatous enterocolitis, and others are less frequent causes of peritoneal infiltration [3]. Epithelial ovarian cancer is the fourth most common cause of cancer death among females in developed countries, in addition to metastasizing through the blood or lymphatic system, ovarian cancer can also spread along the peritoneum [4]. Early detection of peritoneal carcinomatosis is very important to initiate the appropriate oncologic or surgical therapy. Radiological imaging is a valuable tool for guiding treatment management. In this context, the use of PET/CT employing 18F-FDG has been well established for evaluating the biological activity and presence of a suspicious peritoneal nodules and masses, and it has excellent diagnostic performance in the diagnosis of peritoneal carcinomatosis from ovarian cancer [5]. Recognizing the pattern of FDG-avid omental cake is of critical importance in the interpretation of PET imaging in assessing the ovarian cancer.
References
- Canbaz F, Celik H, Kefeli M, Tosun M. Cervical Cancer Presenting as an Omental Cake. Clin Nucl Med. 2018; 43: e417-e418.
- Baratti D, Kusamura S, Deraco M. The Fifth International Workshop on Peritoneal Surface Malignancy (Milan, Italy, December 4-6, 2006): Methodology of disease-specific consensus. J Surg Oncol. 2008; 98: 258-262.
- Basu S, Shet T. FDG avid “abdominal band” representing omental cake in mucinous adenocarcinoma of the appendix: potential implications for disease monitoring with FDG-PET in this setting. J Cancer Res Ther. 2011; 7: 231-3.
- Shijo M, Fukase K, Ohtsuka H, Ariake K, Masuda K, et al. Metastasis of ovarian cancer to the bile duct: A case report. Surg Case Rep. 2019; 5: 100.
- Kim HW, Won KS, Zeon SK, Ahn BC, Gayed IW. Peritoneal carcinomatosis in patients with ovarian cancer: enhanced CT versus 18F-FDG PET/CT. Clin Nucl Med. 2013; 38: 93-97.