
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Diagnostic dilemma in the management of STEMI with anomolous coronary arteries: A case report
Rahul R Gupta; KV Charan Reddy*; Rajesh Matta; Anand Pandhare
Department of Clinical & Interventional cardiology, Apollo Hospitals, Navi Mumbai, India.
*Corresponding Author : KV Charan Reddy
Department of Clinical & Interventional Cardiology, Apollo Hospitals, Navi Mumbai, India.
Email: chrnr@rediffmail.com
Received : Jul 03, 2023
Accepted : Jul 18, 2023
Published : Jul 25, 2023
Archived : www.jcimcr.org
Copyright : © Reddy CKV (2023).
Abstract
Coronary artery anomalies are found in 0.6%-1.55% of patients who undergo coronary angiography. The anomalous origin of the Right Coronary Artery (RCA) as a branch from the Left Anterior Descending artery (LAD) is a very rare variation of the single coronary artery anomaly. Coronary artery anomalies presenting with ST-Segment Elevation Myocardial Infarction (STEMI) are uncommon and challenging to treat. We present a successful Percutaneous Coronary Intervention (PCI) of RCA in a patient who presented with inferior wall myocardial infarction with anomalous RCA arising from proximal LAD. The presentation of this rare coronary anomaly, its pathophysiology, clinical implications and management has been discussed.
Keywords: Coronary artery anomalies; ST-segment elevation myocardial infarction (STEMI); Anomalous RCA arising from LAD.
Citation: Rahul RG, Charan Reddy KV, Rajesh M, Anand P. Diagnostic dilemma in the management of STEMI with anomolous coronary arteries: A case report. J Clin Images Med Case Rep. 2023; 4(7): 2514.
Introduction
The incidence of coronary artery anomalies during coronary angiography is about 1.3% in the largest reported series [1]. A Single Coronary Artery (SCA) is a rare Coronary Artery Abnormality (CAA) where only one coronary artery arises from the aortic trunk by a single coronary ostium, supplying the entire heart. RCA arising from Left Main Coronary Artery (LMCA) with the intra-arterial course has been associated with cardiac ischemia, MI, and sudden death, where as anomalous RCA from mid LAD is reported to be benign. RCA originating from the proximal or mid portion of the left coronary system is extremely rare (with an incidence of 0.009%) [2]. Anomalous coronary artery interventions in STEMI often present with significant anatomical and technical challenges. CAA also poses a diagnostic dilemma especially in a STEMI setting where time is of an essence.
Here, we present a rare type of CAA with the origin of the RCA from LAD in a patient who presented with acute inferior wall STEMI. We also describe the various challenges faced, which necessitated a change in our approach, when encountered with seemingly insurmountable technical challenge. This case also highlights the emphases on planning and flexibility in the thought process needed to safely complete the procedure.
Case presentation
A 35-year-old obese male presented to the ER with retrosternal chest pain and dizziness for the last one hour. He gives a past history of Diabetes, Dyslipidaemia and Hypertension on regular medication. Electrocardiography showed ST elevation in leads II,III and aVF. He was given Aspirin (325 mg), Ticagrelor (180 mg), Atorvastatin (80 mg), intravenous fluids, and immediately shifted to cardiac catheterization lab for primary angioplasty. Transthoracic Echocardiogram (TTE) showed hypokinesia of inferior wall with evidence of right ventricular infarction (tricuspid annular plane systolic excursion-TAPSE of 1.4). LV ejection fraction was 45%, mild mitral and tricuspid regurgitation with no PAH.
Procedure
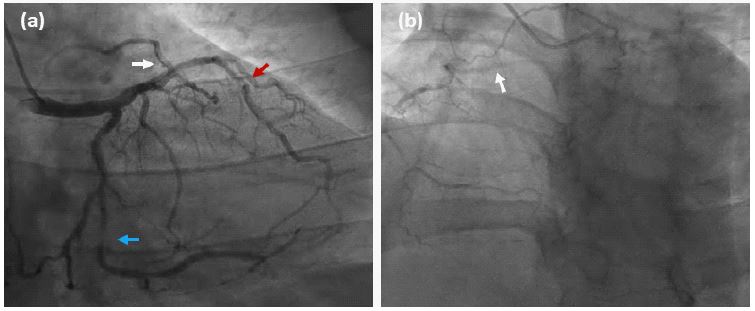
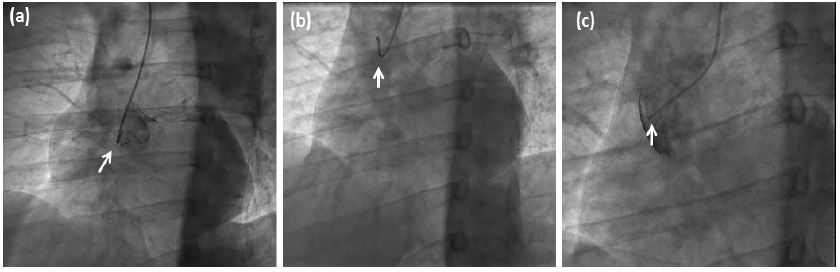
Coronary angiography was performed through the right radial artery. Left Coronary Artery (LCA) was cannulated , which showed critical lesions in the circumflex artery (80%) and mid left anterior descending artery (80%) (Figure 1a,b). A moderate caliber, anomalous and tortuous Right coronary artery was seen originating from the proximal LAD which had near total thrombotic occlusion in the mid segment. An attempt was made to cannulate the right aortic sinus to look for co-dominance of coronary circulation, first with a TIGER, then with AMPLATZ and finally with MULTIPURPOSE diagnostic catheter, without any success (Figure 2a,c). A provisional diagnosis of Single Coronary Artery (SCA) was then made and angioplasty of the culprit artery commenced.
A 6F XB 3.0 guide catheter was used to cannulate the LCA and with the help of a RUNTHROUGH guide wire, the extremely tortuous lesion in the RCA was crossed. However, we noticed severe spasm of the entire RCA which was promptly treated with intracoronary nitroglycerine. Attempts were made to cross the lesion with a 1.5 and 2 mm TAZUNA balloon after wire escalation, without much success. In view of poor guide catheter support and severe spasm of both radial artery and anomalous RCA, the radial approach was abandoned.
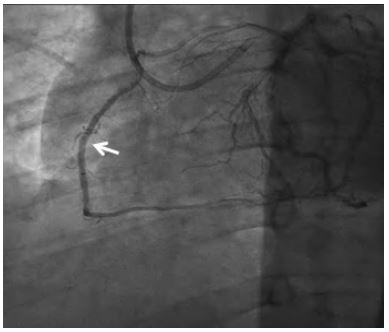
A 7F right femoral artery sheath was placed under USG guidance and LCA cannulated with 7F XB 3.5 guide catheter. This provided a better support for the subsequent balloon dilatations and stent (2.25 x 22 mm ORSIRO DES) placement (Figure 3).
Patient recovered well and was discharged two days later without any complications. CT coronary angiography confirmed the diagnosis of SCA with a benign course of anomalous RCA (anterior to pulmonary artery towards right A-V groove). He later underwent successful angioplasty with stents to LCX and LAD. This case illustrates the importance of planning and anticipation with constant evolution in strategy when facing some seemingly insurmountable obstacles.
Discussion
Congenital Coronary Artery Anomalies (CAA) present from birth are usually asymptomatic and are found incidentally during coronary angiography. Coronary artery anomalies are considered to be the second most common cause of sudden cardiac death among athletes. CAA is found in 0.2 % to 1.3% of patients undergoing coronary angiography and 0.3% at autopsy [3]. The anomalous origin of the RCA is relatively more frequent with a incidence of 0.25% [4]. The anatomic site of anomalous RCA is usually at four locations: Left coronary sinus, antetheca of the aortic wall, supracristal plane above the Right Coronary Sinus (RCS) and left coronary artery system [5,6]. The direction and course of the anomalous RCA is also important. RCA arising from LMCA with interarterial course (between the aorta and the pulmonary artery) is associated with cardiac ischemia, MI, and sudden death, whereas anomalous RCA from proximal or mid LAD and coursing in front of the pulmonary artery is reported to be benign. Due to the long roundabout course of the anomalous RCA, myocardial ischemia can develop even without a definite stenosis. The ectopic origin of long and tortuous RCA can change the hemodynamics of blood flow, leading to various patho-physiological changes in the coronary endothelium, causing vessel spasm and acceleration in atherosclerotic plaque evolution.
Anomalous origin of coronary arteries during primary PCI can give rise to many technical and procedural problems. The duration of PCI is usually longer and associated with increased radiation exposure, to both the patient and operator, with increase in contrast volume. There is also an associated increase in the psychological stress to the operator. Optimal selection and skillful manipulation of guide catheter to maintain coaxiality is the key factor for successful PCI in anomalous RCA. Guide catheters, guidewire and drug eluting stent selection should be based on the location of the RCA ostium, tortuosity and lesion characteristics of the vessel. Judkins left guide or EBU/XB catheters can safely be used to perform PCI in most anomalous RCA cases. However, antetheca or supracristal locations above the coronary sinus, may require Amplatzer left 0.75-1.0 or 3 DRC guide catheters.
In the present case, we encountered many of the problems mentioned above. The presence of small to moderate sized anomalous RCA lead to a search for codominant RCA arising from right aortic sinus. Multiple diagnostic catheters were used without success and it only lead to a increase in procedural time. Inadequate guide catheter support with spasm of the diffusely diseased anomalous RCA, compounded the problems, necessitating a change in the vascular access site, further leading to a delay. Choice of the Drug Eluting Stent (DES) is final piece of the puzzle. A DES with a low crossing profile and a good radial strength (like ORSIRO Ultrathin) should be chosen for easy lesion tracking during complex PCI.
This case emphasizes the need to be at constant lookout and anticipate various problems that may arise when dealing with Coronary Artery Abnormalities (CAA) in a STEMI situation. Knowledge of various hardware and its usage as extension to cardiologist armamentarium, to overcome various complex coronary anatomy, can reduce procedural complications.
Conclusion
Anomalous origin of the Right Coronary Artery (RCA) as a branch from the Left Anterior Descending artery (LAD) is a very rare. RCA arising from LMCA with the interarterial course has been associated with cardiac ischemia, MI, and sudden death whereas anomalous RCA from proximal or mid LAD is usually benign. PCI of anomalous artery is difficult especially in STEMI situations where time is at a premium. The safety of PCI is often guided by the choice of the vascular route taken, guide catheter, guide wires or usage of particular DES. Emphases should be on planning with quick decision making and flexibility in the thought process is needed, to safely complete the procedure.
Conflicts of interest statement: No conflicts of interest.
References
- Gard N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: A coronary arteriographic study. Int J Cardiol. 2000; 74: 39-46.
- Wilson J, Reda H, Gurley JC. Anomalous right coronary artery originating from the left anterior descending artery: Case report and review of the literature. Int J Cardiol. 2009; 137: 195-198.
- Balghith M. Anomalous origin of the right coronary artery from the proximal left anterior descending artery and a single coronary artery anomaly: three case reports. J Saudi Heart Assoc. 2013; 25: 43-6.
- Ho JS, Strickman NE. Anomalous Origin of the Right Coronary Artery from the Left Coronary Sinus: Case Report and Literature Review. Tex Heart Inst J. 2002; 29: 37-39.
- Yurtdas M, Gulen O. Anomalous origin of the right coronary artery from the left anterior descending artery: Review of the literature. Cardiol J. 2012; 19: 122-129.
- Rao U, Agrawal B, Dwivedi S. Anomalous origin of right coronary artery from left coronary sinus. Eur Heart J Cardiovasc Imaging. 2013; 14: 23