
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Original Article - Open Access, Volume 4
Long-term harm associated with renal artery stents in a temporally distant time after the renal function is gone
Charles J Diskin*; Linda M Dansby; Thomas B Carter; Lautrec Radcliff; Charles D Diskin
Hypertension, Nephrology, Dialysis & Transplantation, Edward via School of Medicine at Auburn University, 121 N. 20th Street #20a, Opelika, Al36801, USA.
*Corresponding Author : Charles J Diskin
Hypertension, Nephrology, Dialysis & Transplantation, Edward via School Of Medicine at Auburn University 121 N. 20th Street #20a, Opelika, Al36801, USA.
Tel: 334-742-0242;
Email: HNDT512@bellsouth.net
Received : Aug 02, 2023
Accepted : Aug 22, 2023
Published : Aug 29, 2023
Archived : www.jcimcr.org
Copyright : © Diskin CJ (2023).
Abstract
Introduction: Although large randomized trials have not shown significant benefit of renal artery stent placement, stents continue to be placed in patients with Renal Artery Stenosis (RAS). These intravascular foreign bodies can cause cytokine expression that might result in long-term harm. We evaluated the possibility that they could have adverse effects that were both temporally and spatially distant from their insertion.
Methods: This was a prospective matched pair observational study of 28 patients with RAS initiating chronic maintenance hemodialysis who were paired with patients matched for risk factors of vascular disease. Both groups were evaluated for normality while ANOV, Pearson Correlation, and Cox Proportional Hazards Model were employed to discern significant differences in the need for coronary and peripheral vascular disease intervention, as well as survival.
Findings: The presence of a previous renal artery stent was the most significant risk factor (P = 0.0001) for later development of vascular disease. Patients with renal artery stents had more vascular disease (P = 0.002818), and myocardial infarctions (P = 0.000394), and worse mean survival (42.393 vs 114.730 months).
Conclusion: Despite the previous assumption that renal artery stents do not cause long term complications, it appears that they cause vascular harm and are a significant risk factor for mortality in patients with end stage renal disease on chronic maintenance hemodialysis.
Keywords: Hemodialysis; Renal artery stenosis; Cytokines; End Stage Renal Disease; Vascular Disease; Stents.
Citation: Diskin CJ, Dansby LM, Carter TB, Radcliff L, Diskin CD. Long-term harm associated with renal artery stents in a temporally distant time after the renal function is Gone. J Clin Images Med Case Rep. 2023; 4(8): 2566.
Introduction
While neither the large randomized controlled trials [1,2] nor subsequent subgroup analysis [3] have shown any benefit with respect to renal function or blood pressure for Percutaneous Transluminal Angioplasty (PTA) over medical therapy in patients with RAS, PTA continues to be advocated by guidelines and authors [4]. Justification for this procedure is occasionally made that although benefit may be difficult to demonstrate statistically, the incidence of major complications are low (8.4% - 10%) particularly those permanent (5.8%) [5,6]. Bleeding, artery rupture and acute renal failure are the major problems reported. The focus has therefore been upon the acute post procedural complications; however, we know long term complications might result from the inflammation and cytokines are stimulated by endovascular foreign bodies [7]. That cytokine release and inflammation is now known to increase the expression of endothelial linked adhesion molecules which become a major contributing factor to many vascular events [8,9]. Therefore the presence of an endovascular stent may actually induce the vascular disease it is attempting to treat. Since most endovascular stents are placed in patients with known severe cardiovascular and peripheral vascular disease, it would be difficult to discern which vascular complications have come from the inflammation produced by the stents versus the known underlying severe cardiovascular disease. Does the inflammation contribute to injury beyond the local vessel? Renal artery stents placed for isolated RAS in patients that eventually went to dialysis, however may be a good placed to test the hypothesis that the stent may indeed be harmful years after being placed for RAS since the patient is already in renal failure and renal artery thrombosis and loss of renal function is not an issue. Like other stents, renal artery stents are known to induce an inflammatory response and cytokine production that may be associated with the production of vascular disease. Is that vascular disease localized merely to the vessel with the stent or will it place other vascular beds at risk? In addition, since the ESRD population is particularly prone to vascular inflammatory mediators [10,11], it may be a unique population to test the hypothesis that the inflammation induced by the stent was associated with increased mortality from disease in distant vascular beds. We therefore compared patients who became ESRD who had previously had a renal artery stent with those who had none.
Material and methods
This was a prospective observational study of matched pair design conducted from January 1, 2007 through October 1, 2017. All patients whom had a renal artery stent for an observed RAS and prior to initiation of chronic maintenance hemodialysis were paired upon entry to this observational study with other patients initiating dialysis and matched for the demographics of race, sex, and age as well as risk factors for vascular disease such as: Diabetes, hypertension, chronic inflammatory disease, smoking, hyperlipidemia, use of a statin, use of a proton pump inhibiter (because it can inhibit endothelial nitric oxide) [11], Kt/V, serum albumin, serum hemoglobin, family history of vascular disease or prior known coronary, cerebrovascular or peripheral vascular disease other than the RAS. No patients with angioplasty without a stent were included. All patients who had renal artery stents placed had informed consent to do so. Since we have recently shown that cytokine stimulation has vascular affects in patients who start hemodialysis with an indwelling intravascular catheter [12,13], we also included that as an addition variable for vascular disease. Baseline characteristics of both groups are listed in Table 1. Since it was impossible to completely match an unstented control group without RAS to the stent group as a result there was a bias against the unstented control group without renal artery stenosis. Therefore those with no stents tended to have more vascular risk factors and had several risk factors skewed against that group. Specifically the patients with no stents were more likely to be smokers (P = 0.003) with a chronic inflammatory disease, (e.g. collagen vascular disease, chronic arthritis) (P = 0.008089) who had a family history of vascular disease (P = 0.02) who started dialysis with an indwelling vascular dialysis catheter (P = 0.018636P, but otherwise there were no significant differences at the initiation of dialysis (Table 1).
In Compliance with Ethical Standards: As the work was purely observational by the physicians following the patients after renal failure began and no treatment intervention was either given or withheld by the observers, no other approval was necessary.
Both groups were evaluated by Chi Square and Kolmogorov-Smirnov for normality while ANOV, Pearson Correlation and Cox Proportional Hazards Model were employed to discern significant differences in the need for coronary, and peripheral vascular disease intervention as well as survival.
Results
During the study period, 14 patients started chronic maintenance hemodialysis who had previously placed stents and were matched with 14 other patients matched for the above characteristics but without a renal stent. Of the fourteen patients with stents 12 were bare metal (Medtronic Driver, Cordis Palmaz Blue, Boston Scientific Express) placed a mean of 66.4 months prior to starting dialysis and only two drug eluting (Taxus Liberte, Boston Scientific) placed an average of 92.5 months prior to starting dialysis. Despite all of those variables which should have predisposed the unstented control group without RAS to unfavorable outcomes, in contrast at the conclusion of the study, those with renal artery stents had more vascular disease (P = 0.002818), and myocardial infarctions (P = .000394) (Table 2), and worse mean survival (42.393 vs 114.730 months) (Table 3, Figure 1). While a history of peripheral vascular disease prior to initiating hemodialysis (P = 0.002), diabetes (P = 0.025), a history of coronary artery disease prior to initiating hemodialysis (P = 0.034), and the presence of an indwelling vascular hemodialysis catheter at the initiation of dialysis (P = 0.034) were all significant factors in mortality in the Cox proportional Hazards Analysis; the presence of a previous renal artery stent was the most significant risk factor (P = 0.000) (Table 4). Both groups maintained adequate clearance with an equilibrated Kt/V of 1.5 (NS).
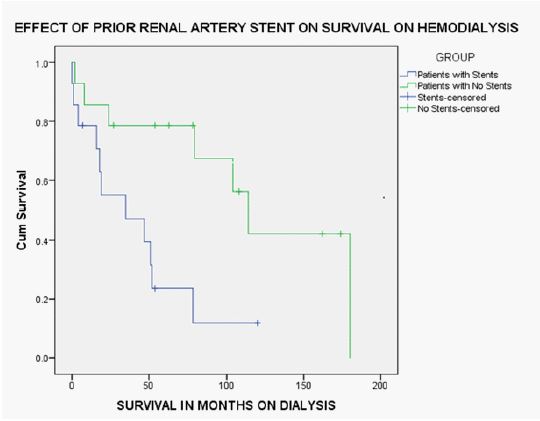
Table 1: Baseline characteristics of the groups studied.
| Stents | No Stent | Significance | |
|---|---|---|---|
| Median Age ± SD | 71 ± 6.6 | 71.5 ± 9.4 | NS |
| Sex (FEMALE/MALE) | 8/6 | 8/6 | NS |
| Race (% WHITE) | 21 | 14 | NS |
| Diabetics | 11 | 14 | NS |
| Hypertension | 14 | 14 | NS |
| Chronic Inflammatory Disorder | 1 | 6 | P = 0.011 |
| Hyperlipidemia | 9 | 10 | NS |
| Median HDL (MG/DL) +/- SD | 37 ± 16.2 | 36 ± 15.6 | NS |
| Median LDL (MG/DL) +/- SD | 73 ± 32.2 | 70 ± 37.7 | NS |
| Statin | 10 | 10 | NS |
| Proton Pump Inhibiter | 10 | 10 | NS |
| Smoking History | 1 | 8 | P = 0.003 |
| Family History Of Vascular Disease | 3 | 8 | P = 0.021 |
| Prior Peripheral Or Cerebrovascular Disease | 2 | 3 | NS |
| Prior Cardioovascular Disease | 4 | 5 | NS |
| Spkt/V | 1.51 ± 0.01 | 1.50 ± 0.02 | NS |
| Median Hemoglobin (G/Dl) (+/- SD) | 10.5 | 10.6 | NS |
| Median Serum Albumin (G/Dl) (+/- SD) | 3.45 | 3.34 | NS |
| Intravascular Dialysis Catheter | 7 | 12 | P = 0.045 |
Before starting hemodialysis, the stent group had fewer risk factors than the unstented control group without renal artery stenosis prior to starting hemodialysis.
Table 2: Vascular events in the groups at conclusion.
| Stents | No Stent | Significance | |
|---|---|---|---|
| Post Stent Peripheral Or Cerebrovascular Disease Events (No. of events) | 2.28 | 0.28 | P = 0.002828 |
| Post Cardiovascular Disease Events (No. Of Events) | 2.5 | 0.14 | P=.0003 |
| Mean Survival (Months) | 29 | 73 | P=0.014 |
| Ekt/V | 1.5 | 1.5 | NS |
After starting hemodialysis, significantly more vascular events developed in the stent group despite a greater number of risk factors in the unstented control group without renal artery stenosis prior to starting hemodialysis.
Table 3: Means and medians for survival time of all patients.
| Group | Meana | Median | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% Confidence Interval | Estimate | Std. Error | 95% Confidence Interval | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Stents | 42.393 | 10.449 | 21.913 | 62.873 | 35.000 | 24.655 | .000 | 83.323 |
| No Stents | 114.730 | 20.808 | 73.945 | 155.514 | 114.000 | 11.998 | 90.483 | 137.517 |
| Overall | 83.035 | 14.421 | 54.769 | 111.301 | 78.000 | 18.924 | 40.908 | 115.092 |
a. Estimation is limited to the largest survival time if it is censored. Survival times were significantly shorter in patients who started dialysis with a renal artery stent, despite the fact that they began dialysis with fewer risk factors than their pair-matched unstented control group without renal artery stenosis. Even if the survival rates of unstented control group without renal artery stenosis were by chance too high, when compared to the overall survival rates of our all 546 patients over the last 5 years median survival was 100.2 months which was not significantly different from unstented control group without renal artery stenosis but was clearly different from those with stents.
Table 4: Cox Proportional Hazards Analysisb
| B | SE | Wald | df | Sig. | Exp(B) | |
|---|---|---|---|---|---|---|
| Presence of Stent | 6.660 | 1.902 | 12.265 | 1 | .000 | .001 |
| Age | .094 | .059 | 2.550 | 1 | .110 | 1.099 |
| Sex | 1.670 | 1.109 | 2.269 | 1 | 132 | 5.311 |
| Diabetes | 3.546 | 1.563 | 5.148 | 1 | .023 | 34.680 |
| Hypertensiona | ||||||
| Chronic Inflammatory Disorder | 2.961 | 1.640 | 3.258 | 1 | .071 | 19.315 |
| Lipids | .051 | 1.508 | .001 | 1 | .973 | 1.052 |
| Statin | -1.565 | 1.480 | 1.117 | 1 | .291 | .209 |
| Smoking | 1.010 | 1.195 | .714 | 1 | .398 | 2.746 |
| FH | .213 | 1.147 | .034 | 1 | .853 | 1.237 |
| Prior PVD | 3.376 | 1.093 | 9.539 | 1 | .002 | 29.244 |
| Prior CAD | 2.017 | .952 | 4.483 | 1 | .034 | 7.513 |
| Perm CATH | 1.794 | .861 | 4.338 | 1 | .037 | 6.014 |
| a. Degree of freedom reduced because of constant or linearly dependent covariates | ||||||
| b. Since all patients had hypertension it became a Constant or Linearly Dependent Covariates HYPERTENSION = 1 | ||||||
While a history of peripheral vascular disease prior to initiating hemodialysis (p = 0.002), diabetes, a history of coronary artery disease prior to initiating hemodialysis, and the presence of an indwelling vascular hemodialysis catheter at the initiation of dialysis were all significant factors in mortality; the presence of a previous renal artery stent was the most significant risk factor.
Discussion
Since the CORAL and ASTRAL studies, the benefit of stents for renal arteries continues to be questioned as the NITER study was not able to show a significant benefit for renal artery stents compared with medical treatment [14] while the ORBITA study [15] has even cast doubt on benefit for coronary arteries; nevertheless, it has always been assumed that they are harmless once past the procedural risk of insertion. Our data casts doubt on that assumption and renal artery stents now may need to be included with indwelling catheters and PTFE as sources of chronic inflammation [16] which may cause vascular harm temporally and spatially remote to a foreign body residing in our renovascular vascular bed. Unlike CORAL and ASTRAL, our study population consisted entirely of dialysis patients in whom the known vascular inflammation of renal failure might be accentuated and therefore produce a much clearer delineation of the effects of the stents. Since the unstented control group without RAS had significantly more variables at the beginning of the study that would are associated with increased risk of vascular disease, one would have expected that the unstented control group without RAS should have developed more vascular disease and had a higher mortality; nevertheless, the presence of vascular disease developed only in patients with stents which was associated with a significantly reduced survival in those with stents. The significance of this data cannot be understated.
Inflammation is now considered central to the pathogenesis of cardiovascular disease [17] and elevated markers of inflammation such as Tumor Necrosis Factor (TNF), and interleukins 1 (IL-1) and 6 (IL-6) have been found to be predictive of future cardiovascular events [18]. While more recently there has been investigation of the role of Danger Associated Molecular Patterns in the pathogenesis of these events [19], the inflammasome with cytokine activation which continues in a central role [18] has long been known to ablate the vascular glycocalyx of heparan sulfate, exposing Endothelial Linked Adhesion Molecules (ELAM) which attract platelet aggregation [20]. Although hemodialysis is known to reduce IL-8 [21], stents are known to increase CRP, TNF, IL-6, and Il-8 [22], whether the stents are bare metal or drug eluting [23]. Therefore stents appear to activate systemic inflammation [24,25] and therefore have a tendency to exacerbate the inflammatory conditions [26] already known to occur in the vasculature in renal failure [27]. Given that the prevalence of peripheral vascular disease in patients on dialysis is 34 percent [28] and that cardiovascular disease is 69.6 percent among persons ages 66 and older who have chronic renal disease, compared to 34.7 percent among those who do not [29], the presence a stent in the renal arteries may be less than unhelpful. Our data would suggest that those patients with renal artery stents who develop end stage renal disease and require dialysis develop more significant vascular disease, even if they have fewer traditional risk factors at the onset of dialysis.
Some potential limitations to our study would include the smaller size and effect of hemodialysis. The effect of size we would suggest is somewhat mitigated by the matched pair design. Some have previously suggested that RAS is a potent marker for patients who will eventually develop severe disease and consequently would eventually suffer worse outcomes. Therefore concluding that the stent itself caused the worse outcomes would be analogous to blaming insulin for the higher amputation rate for patients with insulin-dependent diabetes. We do not think the medical literature supports that viewpoint any longer. More recent studies performed after ASTRAL have suggested a lack of association of RAS with increased mortality [30]. Similarly RAS in patients undergoing coronary artery bypass grafting without the use of stents are also not associated with increased mortality [31], while stenting still results in higher mortality and vascular disease [32]. Nevertheless, previous works prior to ASTRAL when renal artery stenting was more common suggested that RAS is associated with increased mortality but that increased mortality is usually associated with increased traditional risk factors in patients with age, diabetes [33,34], smoking [33], and existing vascular disease [33,34]. existing cardiac disease [32-34], hypertension [33-35] and renal function, [33-35] particularly after angioplasty and stenting [34-37]. The increased mortality with stenting in RAS was then determined not to be related to acute complications and post-operative mortality but was indeed much more of a long term problem [35]. Additionally in a study of 51 patients with RAS who were left unstented six eventually went to dialysis and were associated with excessive mortality [38]. Unfortunately since RAS is associated with increased progression to renal failure no one has ever been able to control for that variable. In contrast to that data, our study controlled for all known traditional risk factors (Table 1) and in fact placed higher amounts of known vascular disease in the unstented group; but in addition we controlled for renal function. Renal failure alone predisposes patients to vascular disease [28], through intense inflammation which is not affected by the modality of dialysis [38]. Therefore it should be expected that those patients who went to end stage renal disease should have a higher incidence of vascular disease and mortality as was found in the work of Baboolal [39]. That is why our study is so unique since we only look at vascular disease and mortality under the same clinical situation of end stage renal disease in both stented and unstented patients without stenosis on dialysis where the influence of the inflammatory effect of renal failure is present equally in both groups, while the unstented patients are given the higher number of traditional risk factors (Table 1). Despite fewer traditional risk factors, the stented group developed more cerebrovascular, cardiovascular and peripheral vascular events which resulted in a much higher mortality rate. Therefore our study is consistent with current literature which suggests that the stent itself rather than the renovascular disease seems to herald increased cardiovascular morbidity and mortality.
It should be noted that soluble thrombomodulin, osteopontin and soluble tumor necrosis factor receptor-2 are linked to vascular inflammation and remodeling while endothelial lipase activity may control high density lipoproteins( HDL) [40] that can ameliorate inflammation [41]; however, we have no data on those biomarkers. Nonetheless there were no differences in HDL levels between the unstented control group without RAS and the patients with stents (Table 1). On the other hand, hemodialysis reduces cytokine concentrations and patients who undergo long nocturnal quotidian dialysis were shown to have greater improved concentration levels of cytokines [42]; however, all of our patients underwent traditional thrice weekly hemodialysis with an identical mean Kt/V. Whether long nocturnal quotidian hemodialysis could mitigate the inimical effects of the indwelling stents through decreased inflammation or perhaps even other mechanisms [43] could be an area for future research. Also, we hope our study urges future research in renal artery stents’ harmful long-term effects in patient populations other than end stage renal disease.
Conclusion
Despite the previous assumption that renal artery stents do not cause long-term complications, it appears that they might cause longer-term vascular harm and be a significant risk factor for mortality in patients with end stage renal disease on chronic maintenance hemodialysis. While this study would not have been possible to perform with coronary stents since the vascular disease would have already involved a vital organ, we could do this study on renal artery stents since dialysis would serve excretory functions to allow our surveillance of the progression of atherosclerosis. In the dialysis patients, vascular disease progressed much faster in the stented patients despite having a lower burden of disease and risk factors at the onset. Unfortunately, our data is merely preliminary and only a truly randomized controlled study with full measurements of the involved cytokines will answer this question. Since the answer would potentially involve a major change in the way we view the treatment of vascular disease, we hope that this initial study will be the impetus for such a future endeavor.
References
- ASTRAL Investigators, Wheatley K, Ives N, Gray R, Kalra PA, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009; 361: 1953-62
- Cooper CJ, Murphy TP, Cutlip DE, Jamerson K, Henrich W, et al. CORAL Investigators. Stenting and medical therapy for atherosclerotic renal-artery stenosis N Engl J Med. 2014; 370: 13-22.
- Ritchie J, Green D, Chrysochou T, Hegarty J, Handley K, et al. Effect of renal artery revascularization upon cardiac structure and function in atherosclerotic renal artery stenosis: Cardiac magnetic resonance sub-study of the ASTRAL trial. Nephrol Dial Transplant. 2017; 32: 1006-1013.
- Tafur JD, White CJ. Renal Artery Stenosis: When to Revascularize in 2017. CurrProblCardiol. 2017; 42: 110-135.
- Ivanovic V, McKusick MA, Johnson CM 3rd, Sabater EA, Andrews JC, et al. Renal artery stent placement: complications at a single tertiary care center. J Vasc Interv Radiol. 2003; 14: 217-25.
- Beek FJ, Kaatee R, Beutler JJ, van der Ven PJ, Mali WP. Complications during renal artery stent placement for atherosclerotic ostial stenosis. Cardiovasc Intervent Radiol. 1997; 20: 184-90.
- Roy-Chaudhury P, Kelly BS, Miller MA, Reaves A, Armstrong J, et al. Venous neointimal hyperplasia in polytetrafluoroethylene dialysis grafts. Kidney Int. 2001; 59: 2325-34.
- Sullivan GW, Sarembock IJ, Linden J. The role of inflammation in vascular diseases. J Leukoc Biol. 2000; 67: 591-602.
- Mohsen M, Narges, Habib H, Mahmood M, Najmaldin S. Inflammatory Growth Factors and In-Stent Restenosis: Effect of Cytokines and Growth Factors SN Compr Clin Med. 2020; 1-2.
- Chong KC, Owens CD, Park M, Alley HF, Boscardin WJ, et al. Relationship between kidney disease and endothelial function in peripheral artery disease. J Vasc Surg. 2014; 60: 1605-11.
- Papayianni A, Alexopoulos E, Giamalis P. Circulating levels of ICAM-1. VCM-1.and MCP-1 are in-creased in haemodialysis patients association with inflammation dyslipidaemia and vascular events. Nephrol Dial Transplant. 2002; 17: 435-41.
- Pinheiro LC, Oliveira-Paula GH, Portella RL, Guimarães DA, de Angelis CD. Tanus-Santos JE Omeprazole impairs vascular redox biology and causes xanthine oxidoreductase-mediated endothelial dysfunction. Redox Biol. 2016; 9: 134-143.
- Diskin CJ, Stokes TJ, Dansby LM, Radcliff L, Carter TB, et al. The first fistula: influence of location on catheter use and the influence of catheter use on maturation. Int Urol Nephrol. 2015; 47: 1571-5.
- Siddiqui EU, Murphy TP, Naeem SS, Siddique A, McEnteggart GE, et al. Interaction between Albuminuria and Treatment Group Outcomes for Patients with Renal Artery Stenosis: The NITER Study.J Vasc Interv Radiol. 2018; 29: 966-970.
- Al-Lamee R, Thompson D, Dehbi H, et al. Percutaneous coronary intervention in stable angina (ORBITA): a double blind, randomised controlled trial. Lancet. 2017.
- Sachdeva M, Hung A, Kovalchuk O, Bitzer M, Mokrzycki MH. The initial vascular access type contributes to inflammation in incident hemodialysis patients. Int J Nephrol. 2012; 2012: 917465
- Ruparelia N, Chai JT, Fisher EA, Choudhury RP. Inflammatory processes in cardiovascular disease: a route to targeted therapies Nat Rev Cardiol. 2017; 14: 133-144.
- Biasucci LM, Liuzzo G, Fantuzzi G, Caligiuri G, Rebuzzi AG et al. Increasing levels of interleukin (IL)-1Ra and IL-6 during the first 2 days of hospitalization in unstable angina are associated with increased risk of in-hospital coronary events. Circulation. 1999; 99: 2079-2084.
- Biasucci LM, La Rosa G, Pedicino D, D’Aiello A, Galli M, et al. Where Does Inflammation Fit? Curr Cardiol Rep. 2017; 19: 84.
- Diskin CJ, Stokes TJ, Dansby LM, Radcliff L, Carter TB. Understanding the pathophysiology of hemodialysis access problems as a prelude to developing innovative therapies. Nat Clin Pract Nephrol. 2008; 4: 628-38.
- Tarakçioğlu M, Erbağci AB, Usalan C, Deveci R, Kocabaş R. Acute effect of hemodialysis on serum levels of the proinflammatory cytokines. Mediators Inflamm. 2003; 12: 15-9.
- Caixeta AM, Brito FS Jr, Costa MA, Serrano CV Jr, Petriz JL, et al. Enhanced inflammatory response to coronary stenting marks the development of clinically relevant restenosis. Catheter Cardiovasc Interv. 2007; 69: 500-7.
- Gogo PB, Schneider DJ, Watkins MW, Terrien EF, Sobel BE, et al. Systemic Inflammation after Drug-Eluting Stent Placement. J Thromb Thrombolysis. 2005; 19: 87.
- Almagor M, Keren A, Banai S. Increased C-reactive protein level after coronary stent implantation in patients with stable coronary artery disease. Am Heart J. 2003; 145: 248-53.
- Walter J Gomes. Enio BuffoloCoronary stenting and inflammationRev Bras Cir Cardiovasc. 2003; 18.
- Sánchez-Margalet V, Cubero JM, Martín-Romero C, Cubero J, Cruz-Fernández JM, et al. Inflammatory response to coronary stent implantation in patients with unstable angina. Clin Chem Lab Med. 2002; 40: 769-74.
- Batko K, Krzanowski M, Gajda M, Dumnicka P, Fedak D, et al. Endothelial injury is closely related to osteopontin and TNF receptor-mediated inflammation in end-stage renal disease. Cytokine. 2019; 121: 154729.
- USRDS Annual Data Report. Cardiovascular Disease in patients with ESRD. 2017.
- https: //www.niddk.nih.gov › Health Information › Health Statistics. 2019.
- Aboyans V, Desormais I, Magne J, Morange G, Mohty D, et al. Renal artery stenosis in patients with peripheral vascular disease: Prevalance, risk factors and long-term prognosis. Eur J Vasc Endovasc Surg. 2017; 53: 380-5.
- Aboyans V, Tanguy B, Desormais I, Bonet V, Chonchol M, et al. Prevalence of renal artery stenosis and its prognostic significance in patients undergoing coronary artery bypass grafting Am J Cardiol. 2014; 114: 1029-34.
- Kiriyama H, Kodera S, Minatsuki S, Kaneko H, Kikuchi H, et al. Short-Term and Long-Term Efficacy of Drug-Coated Balloon for In-Stent Restenosis in Hemodialysis Patients with Coronary Artery Disease. Int Heart J. 2019; 60: 1070-1076.
- Mui KW, Sleeswijk M, van den Hout H, van Baal J, Navis G, et al. Incidental renal artery stenosis is an independent predictor of mortality in patients with peripheral vascular disease. J Am Soc Nephrol. 2006; 17: 2069-74.
- Valentine RJ, Myers SI, Miller GL, Lopez MA, Clagett GP. Detection of unsuspected renal artery stenoses in patients with abdominal aortic aneurysms: Refined indications for preoperative aortography. Ann Vasc Surg. 1993; 7: 220-224.
- Conlon PJ, Athirakul K, Kovalik E, Schwab SJ, Crowley J, et al. Survival in renal vascular disease. J Am Soc Nephrol. 1998; 9: 252-6.
- Mui KW, Zeebregts CJ, van den Hout H, van Baal J, Navis G, et al. Impact of incidental renal artery stenosis on long-term mortality in patients with peripheral vascular disease undergoing a vascular procedure. J Vasc Surg. 2011; 54: 785-790.
- Bonelli FS, McKusick MA, Textor SC, Kos PB, Stanson AW, et al. Sheedy PF 2nd, Welch TI: Renal artery angioplasty: Technical results and clinical outcome in 320 patients. Mayo Clin Proc. 1995; 70: 1041-1052.
- Baboolal K, Evans C, Moore RH. Incidence of end-stage renal disease in medically treated patients with severe bilateral atherosclerotic renovascular disease. Am J Kidney Dis. 1998; 31: 971-7.
- Borràs Sans M, Pérez-Fontán M, Martinez-Alonso M, Bajo A, Betriu À, et al. The modality of dialysis does not influence atheromatous vascular disease progression or cardiovascular outcomes in dialysis patients without previous cardiovascular disease. PLoS One. 2017; 12: e0186921
- Miksztowicz V, McCoy MG, Schreier L, Cacciagiú L, Elbert A, et al. Endothelial lipase activity predicts high-density lipoprotein catabolism in hemodialysis: Novel phospholipase assay in postheparin human plasma. Arterioscler Thromb Vasc Biol. 2012; 32: 3033-40.
- Cacciagiú LD, González AI, Gomez Rosso L, Meroño T, De Marziani G, et al. HDL-associated enzymes and proteins in hemodialysis patients. Clin Biochem. 2012; 45: 243-8
- Yuen D, 23. Richardson RM, Fenton SS, McGrath-Chong ME, Chan CT. Quotidian nocturnal hemodialysis improves cytokine profile and enhances erythropoietin responsiveness. ASAIO J. 2005; 51: 236-41.
- Chan CT, Harvey PJ, Böger R, Pierratos A, Floras JS. Dissociation between the short-term effects of nocturnal hemodialysis on endothelium dependent vasodilation and plasma ADMA. Arterioscler Thromb Vasc Biol. 2005; 25: 2685-6.