
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Reverse takotsubo after emotional distress and catecholamine bolus
Giglio Andres1,2*; Revello Javier3; Garcia Francisca1; Aguilera Fabian3; Ramirez Paulina3; Hoffmann Isabel3
1School of Medicine, Universidad Finis Terrae, Chile.
2Critical Care Unit, Clinica Las Condes, Chile.
3Internal Medicine Department, Complejo Asistencial Dr. Sotero del Río, Chile.
*Corresponding Author : Giglio Andrés
Critical Care Program, Universidad Finis Terrae, Chile.
Email: agiglioj@gmail.com
Received : Sep 11, 2023
Accepted : Sep 26, 2023
Published : Oct 03, 2023
Archived : www.jcimcr.org
Copyright : © Andrés G (2023).
Citation: Andres G, Javie R, Francisca G, Fabian A, Paulina R. et al. Reverse takotsubo after emotional distress and catecholamine bolus. J Clin Images Med Case Rep. 2023; 4(10): 2626.
Clinical image description
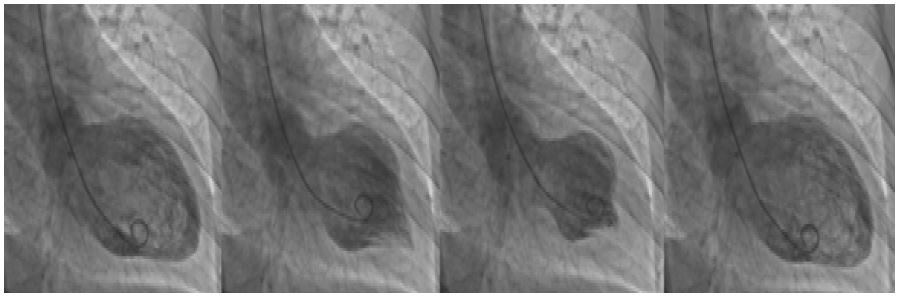
A patient in his 40s was referred from a primary care facility to the emergency department because of chest pain, hypotension which was managed with a bolus of adrenaline, and diffuse ST depression on electrocardiography (ECG) after a life event with a high emotional impact. The patient was admitted with persistent hypotension and a second ECG with persistent ST depression; however, isobiphasic T was observed in some of the precordial leads. Given the evolving ECG, thoracic pain, and elevated troponin levels, the patient was admitted for percutaneous coronary angiography (PCI), considering the risk of Acute Coronary Syndrome. The latter reports coronary arteries without lesions but ventriculography with reverse Takotsubo morphology (Figure 1).
Takotsubo cardiomyopathy is described as left ventricular dysfunction triggered by emotional or physical stress, seen predominantly in women (90%), with a median age of 66 years [1]. The reverse morphology accounts for a variable range from to 1-23% of all Takotsubo [2], being 2.2% in the International Takotsubo Registry [1,3], and is associated with younger age and less decrease in left ventricular ejection fraction [2]. The pathophysiology of this entity, or the cause of the reverse morphology, is still uncertain, even though theories such as the beta receptor gradient transition from basal distribution in the young to apical distribution in the elderly, are possible explanations [3].
References
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. New England Journal of Medicine. 2015; 373(10): 92938.
- Awad HH, McNeal AR, Goyal H. Reverse Takotsubo cardiomyopathy: a comprehensive review. Ann Transl Med. 2018; 6(23): 460-460.
- Rashed A, Shokr M, Subahi A, Siddiqui F, Alkatib A, Afonso L. Reverse takotsubo cardiomyopathy in a patient with prior apical takotsubo cardiomyopathy: Challenging the beta receptor gradient theory. Ochsner Journal. 2019; 19(3): 256-9.