Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Intestinal endometriosis: A rare clinical image of sigmoid presentation
Safak Kiziltas; Mert Doruk Bal*
Department of Internal Medicine, Acibadem Mehmet Ali Aydinlar University School of Medicine, Istanbul, Turkey.
*Corresponding Author : Mert Doruk Bal
Department of Internal Medicine, Acibadem Mehmet Ali Aydinlar University School of Medicine, Istanbul, Turkey.
Email: mrtdrkbl@hotmail.com
Received : Oct 12, 2023
Accepted : Nov 10, 2023
Published : Nov 17, 2023
Archived : www.jcimcr.org
Copyright : © Bal MD (2023).
Citation: Kiziltas S, Bal MD. Intestinal endometriosis: A rare clinical image of sigmoid presentation. J Clin Images Med Case Rep. 2023; 4(11): 2696.
Clinical image description
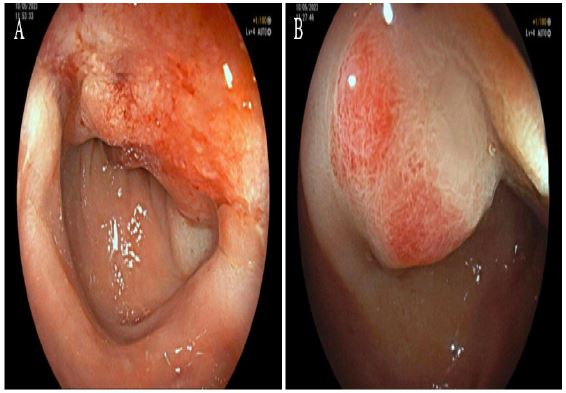
A 47-year-old female patient with a history of umbilical endometriosis and iron deficiency anemia presented to the gastroenterology department with a year-long complaint of abdominal pain, rectal pain, and hematochezia during menstruation. The physical examination and the results of laboratory studies of the patient were unremarkable. A contrast MRI of the abdomen revealed pathological thickening of 1.5 cm in the middle segment of the rectum and chocolate cysts on both ovaries, and the patient was referred for colonoscopic evaluation with suspicion of infiltrative endometriosis or colon neoplasm. An upper endoscopy and colonoscopy were performed. An actively bleeding mass in sigmoid colon, partially restricting the lumen but allowing for the passage of the video colonoscope, was observed (Figure 1A,1B: Sigmoid lesion). Biopsy specimens from the sigmoidal mass showed features consistent with endometriosis. A diagnosis of endometriosis was made. The patient underwent surgical intervention by sigmoid colon resection, hysterectomy, and bilateral oophorectomy. The complaints ceased on postoperative follow-up.