
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Iris cyst and myelinated retinal nerve fibers about a case: Real or accidental association?
El Hadji Malick SY*; Soda Mbaye; Aissatou AW; Jean Pierre Diagne; Ousmane Ndiaga Senghor; Serigne Sohibou Gaye; Mouhamed Ndiaye; El Hadj Abdellahi Seyid; Aly Mbara Ka; Papa Amadou Ndiaye
Abass-Ndao-de-Dakar Hospital, Dakar, Sénégal.
*Corresponding Author : El Hadji Malick SY
Abass-Ndao-de-Dakar Hospital, Dakar, Sénégal.
Email: elhadjimalicksyonly@gmail.com
Received : Oct 31, 2023
Accepted : Nov 29, 2023
Published : Dec 06, 2023
Archived : www.jcimcr.org
Copyright : © Malick SYH (2023).
Citation: Malick SYH, Mbaye S, Aissatou AW, Diagne JP, Senghor ON, et al. Iris cyst and myelinated retinal nerve fibers about a case: Real or accidental association?. J Clin Images Med Case Rep. 2023; 4(12): 2724.
Introduction
Iris cysts are rare conditions whose differentiation between primary and secondary involvement depends essentially on clinical presentation. According to the classification, primary cysts are those developed at the expense of the pigment iris epithelium, stroma or free-floating cyst. Secondary cysts are usually due to trauma, surgery of the anterior segment or more rarely to a melanocytic tumor of the anterior segment [1].
Myelinated Retinal Nerve Fibers (MRNF) are congenital or acquired abnormalities of myelination [2,3]. They were described for the first time by Virchow in 1856, in the form of whitish plates finely striated at the blurred edge and located at the layer of the optical fibers, at a distance or contiguous to the papilla [2].
The association between iris cyst and MRNF is a rare entity and only one case has been reported in the literature by Shields [4].
Faced with the rarity of this entity and the question to know would it be a fortuitous or real association? We share this case of primary iris cyst associated with MRNF.
Observation
He was a 41-year-old man, with no pathological medical history, no notion of trauma or eye surgery, referred for iris neoformation in the left eye.
The ophthalmological examination showed a corrected visual acuity at 8/10e P2 to the right eye and a left eye at 10/10e P2.
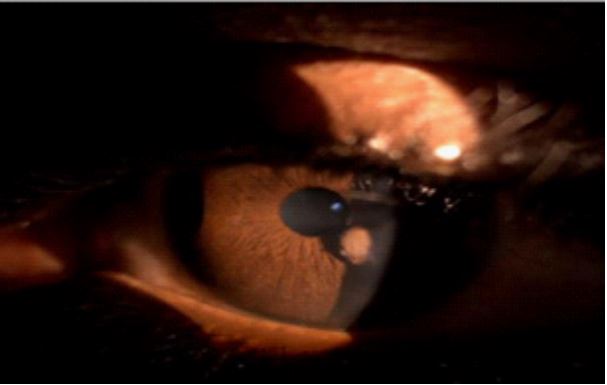
Examination of the anterior segment of the right eye was normal. In the left eye, we found a single, rounded, pigmented, inferior-temporal iridescent mass, about 2 millimeters (mm) in diameter, cystic in appearance, developing at the expense of the iris epithelium and not covering the pupil (Figure 1). Intraocular pressure was normal in both eyes.
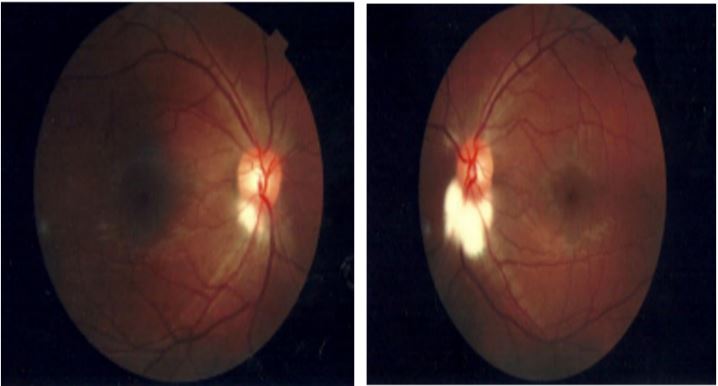
At the bottom of the eye, we find a whitish closet, plane, located in inferior-temporal of the optic papilla, with scalloped edges to both eyes but more marked to the left eye.
Retinography confirmed the fundus results and suggested myelinated fibers to both eyes (Figures 2a and 2b).
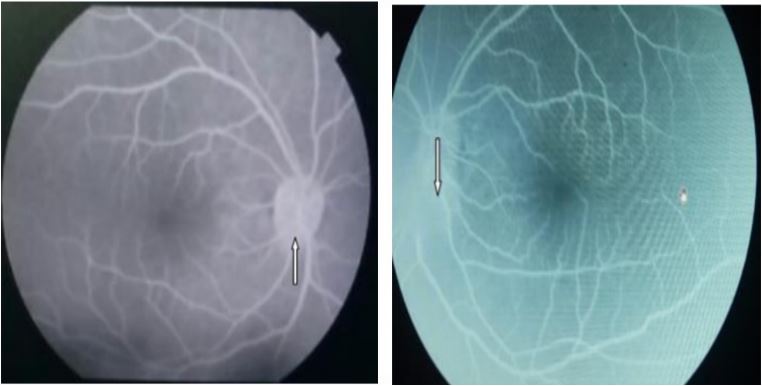
Fluorescein angiography showed a “mask effect” in the inferior-temporal zone of both eyes corresponding to the localization of myelinated fibers (Figures 3a and 3b).
Optical Coherence Tomography (OCT) showed no particular abnormalities apart from a thickening of the myelin fiber area.
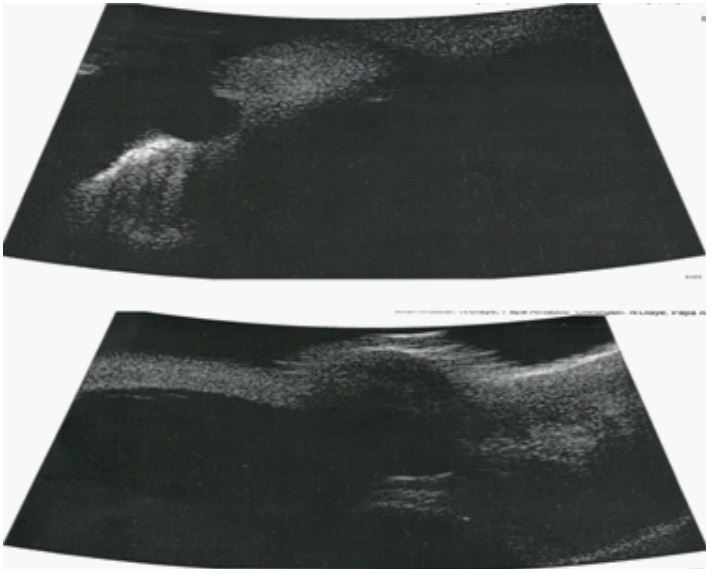
Ultrabiomicroscopy (UBM) confirmed the cystic nature of the iris mass with a thick, hyperechoic wall and anechoic content. The posterior limits of the cystic pocket were not visible (Figure 4).
Before this clinical picture, the diagnosis of primary cyst of the left pupillary pigment epithelium associated with bilateral MRNF was retained. The recommended treatment in our patient was a therapeutic abstention and a progressive monitoring of objectified lesions.
After regular follow-up at first semi-annual and then annual until now, the patient had not presented any progression of lesions or complications related to these disorders.
Discussion
The iris cyst is a rare benign condition with a central form representing only 3% of primary attacks [5,6]. In their retrospective studies of about twelve years for Shields [5] and twenty years for Lois [6], they found respectively 62 and 234 cases of iris cysts. In our practice, this is the first known iris cyst case.
The morphology of iris cysts is essentially marked by a wall of varying thickness and echogenicity, always continuing with the pigment epithelium. This extension with the iris pigment epithelium is the reason for its frequent confusion with the melanomas of the ciliary body [6-8]. This is also believed to be the cause of several reported cases of enucleation on eyes with an iris cyst [6]. The advent of UBM revolutionized diagnostic and therapeutic management and allowed a better individualization of the structures of the anterior segment (iris, angle or ciliary body) [8].
Some authors consider iris cysts as serious according to their position (stroma and pigment epithelium) or complications caused such as angle closure glaucoma, plateau iris syndrome, pigment deposits in the trabeculum, cataracts, subluxation or inflammation of the corneal endothelium [6-8]. It has also been described a pathological combination of iris cysts and aortic dissection. It is imperative to look for a cardiopathy (aortic dissection) associated with multiple iris cysts [9,10].
MRNF, unlike iris cysts are often associated with other ocular pathologies. In the majority of their association, they are involutive and disappear later after optical atrophy secondary to treatment [11,12]. Numerous studies report the association of MRNF with retinal vascular abnormalities, myopia, amblyopia, strabismus, vitreoreretinopathy or more rarely skeletal malformations [13-15].
In the literature, only one case of association between an iris cyst and MRNF has been reported [5]. It is a rare and essentially unknown pathological entity. Among the physiopathological explanations, embryological theory seemed to be the most plausible. Indeed, she argues that in the image of the pigment iris epithelium, the retinal also has an ectoblast origin and therefore an embryological malformation of one of the epithelia would probably be found in the other justifying the association between these two disorders. However, the mechanism of the genesis of MRNF, which would be related to the screened blade, excludes any involvement of the ectoblast and refutes this theory [16]. The presence of bilateral MRNF suggests a probable genetic origin [17]. Of two reported family cases of bilateral MRNF, Funnel suggested the probable existence of a genetic factor [17]. In our patient the genetic investigation had noted an absence of inbreeding or similar cases in the family. However, given the bilateral involvement of MRNF and their association with a unilateral central iris cyst, a genetic assessment (genomic sequencing) would be more appropriate to eliminate or confirm this theory.
Iris cysts and my MRNF are often asymptomatic pathologies and accidental discovery [2,7]. In the various studies on iris cysts, only one case associating the two attacks, had been recorded [5,6]. This rarity of the association could be linked on the one hand by the absence of large-scale study and on the other hand to the fact that it is likely to be under-diagnosed with the almost total absence of functional signs related to one or the other pathology.
Therapeutically, the management of these two pathologies is different. For cysts, their treatment would depend on the authors of their location and their symptomatology. Thus cases of symptomatic iris cysts were treated by argon laser or surgical excision without recurrence and with simple postoperative follow-ups [6,7]. In contrast, Shields considered the iris cysts as an ophthalmological curiosity, advocated for their management a therapeutic abstention [5]. Moreover, regarding MRNF, the authors agree that simple surveillance would be sufficient without any complications [2]. In our patient, the surveillance and the therapeutic abstention were preferred before the absence of symptomatology. The evolution in our case, was marked by a stationary state of the lesions after several years of clinical and iconographic surveillance.
Given the lack of significant correlation between these two disorders and a precise pathophysiology and according to the data of the literature, this association of iris cyst and MRNF is a fortuitous association and would be of pure coincidence.
Conclusion
Iris cyst and myelinated retinal nerve fibers layers are rare and essentially asymptomatic. The discovery of multiple iris cysts must systematically seek cardiac involvement such as aortic dissection, which is an emergency that can affect the patient’s vital prognosis. The diagnosis of bilateral myelinated retinal nerve fibers layers should look for similar cases in the family and suggest a genetic investigation. Despite their common embryological origin between the two epithelia, the association of iris cyst and myelinated retinal nerve fibers layers is a pathological coincidence of chance discovery and stable evolution. However, genetic theory could be an avenue to explore in order to allow a pathophysiological determination.
References
- Van Haren C, Ozturk N, De Potter P, et al. Kyste d’inclusion épithéliale irien: A propos d’un cas. J Fr Ophtalmol. 2022; 45: e438-40.
- Velasque L, Mortemousque B. Les fibres à myéline rétiniennes; Revue de la littérature à propos d’un cas. J Fr Ophtalmol. 2000; 23: 892-996.
- Prakalapakorn SG, Buckley MPH. Buckley EG. Acquired bilateral myelinated retinal nerve fibers after unilateral optic nerve sheath fenestration in a child with idiopathic intracranial hypertension. JAAPOS. 2012; 16: 534-8.
- Shields JA, Kline MW, Augsburger JJ. Primary iris cysts: A review of the literature and report of 62 cases. Br J Ophtalmol. 1984;68: 152-66.
- Shields JA. Primary iris cysts. Trans Am Ophthalmol Soc. 1981; 79: 771-809.
- Lois N, Shields CL, Shields JA. et al. Primary Cysts of the Iris Pigment Epithelium. Clinical Features and Natural Course in 234 Patients. Ophthalmology. 1998; 105: 1879-85.
- Dammacco R, Giancipoli G, Guerriero S, et al. Primary pupillary margin cyst of the Iris pigment epithelium. Chinese Medicine. 2011, vol 2, p. 16-9.
- Roche O, Orssaud C, Beby F, et al. Ultrabiomicroscopie et physiopathologie des kystes iriens congénitaux. J Fr. Ophtalmol. 2007; 30: 25-30.
- Hashida N, Ohguro N, Morimoto Y. Ultrastructural appearance of iris floccule associated with a thoracic aortic aneurysm and dissections. Br J Ophtalmol. 2009; 93: 1409-10.
- Phowthongkum P, Burapasubkajorn P, Intarabeth P. Familial Aortic Dissection and Congenital Iris Floccule with Hypertention. Opthalmic Genetics. 2008; 29: 126-7.
- Mashayekhi A, Shields CL, Shields JA. Disappearance of Retinal Myelinated Nerve Fibers after Plaque Radiotherapy for Choroidal Melanoma. The journal of retinal and vitreous diseases. 2003; 23: 572-3.
- Katz SE, Weber PA. Photographic documentation of the loss of medullated nerve fibers of the retina in uncontrolled primary open angle glaucoma. J Glaucoma. 1996; 5: 406-9.
- Leys AM, Leys MJ, Hoymaans JMM. Myelinated Nerve Fibers and Retinal Vascular Abnormalities. The journal of retinal and vitreous diseases. 1996; 16: 89-96.
- Tarabishy AB, Terry JA, Traboulsi EI. Syndrom of Myelinated Retinal Nerve Fibers, Myopia, and Amblyopia: A Review. Surv Ophtalmol. 2007; 52: 588-96.
- Traboulsi EI, Lim JI, Pyeritz R, et al. A new syndrom of myelinated nerve fibers, vitreoretinopathy, and skeletal malformation. Arch Ophtalmol. 1993; 111: 1543-5.
- Williams TD. Medullated Retinal Nerve Fibers: Speculations on Their Cause and Presentation of Cases. Am J Optom Physiol Opt. 1986; 63: 142-51.
- Funnell CL, George NDL, PAI V. Familial myelinated retinal nerve fibres. Eye London. 2003; 17: 96-7.