
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Asymptomatic pulmonary co-infection with Cryptococcus and Aspergillus in a patient from China
Xinyan Du; Li Yang; Jianrong Luo; Yi Zhong; Fengling Chen*
Department of Laboratory Medicine, Medical Center Hospital of Qionglai City, Chengdu 611530, Si chuan, China.
*Corresponding Author : Fengling Chen
Department of Laboratory Medicine, Medical
Center Hospital of 172 Xinglin Road, Qionglai City,
Sichuan Province, China.
Email: selina_chenxiaoyi@163.com
Received : Nov 11, 2023
Accepted : Dec 07, 2023
Published : Dec 14, 2023
Archived : www.jcimcr.org
Copyright : © Chen F (2023).
Abstract
An asymptomatic HIV-negative patient was admitted to hospital because she was found multiple pulmonary nodules by chest Computed Tomography (CT) in a routine examination. And the patient was diagnosed as pulmonary cryptococcosis and aspergillosis not cancer by percutaneous lung biopsy and special tissue stain. At last, patient was administrated with surgery and continuous antifungal therapy to eliminate pulmonary nodules, and the negative results of serum Cryptococcus and Aspergillus antigen indicated a favorable prognosis.
Keywords: Cryptococcus neoformans; Aspergillus; Pneumonia; Computed tomography.
Citation: Du X, Yang L, Luo J, Zhong Y, Chen F. Asymptomatic pulmonary co-infection with Cryptococcus and Aspergillus in a patient from China. J Clin Images Med Case Rep. 2023; 4(12): 2736.
Introduction
Cryptococcus is a yeast-like fungus encapsulated with polysaccharide that exists mostly in bird droppings, polluted soil, decayed plant materials and granary. There are four serum types (A-D types) about Cryptococcus that is frequently seen in immunocompromised population like Acquired Immune Deficiency Syndrome (AIDS) patients, and cryptococcosis is the second major cause of AIDS-related mortality worldwide, besides, B and C types are verified to have risk of opportunistic infection for immunocompetent human [1-3]. Apart from AIDS, Immunodeficiency related diseases still include solid-organ transplantation, diabetes, malignant neoplasm, cirrhosis and immunosuppressive state, which are risk factors for infection [4-6]. Typical symptoms of cryptococcosis include cryptococcal meningitis, pulmonary nodule and skin ulcer. The patient had pulmonary nodules. Aspergillosis is an epidemic disease that spreads via polluted air or dust in humid environment and an also opportunistic pathogen and so it is rare for infection to normal people. Typical symptoms of aspergillosis is tuberculoid change in lung like this patient, but she had no obvious blood inflammatory response. It is a challenge for diagnosis of infection that there was no typical symptom. Moreover, there are few case reports about non-HIV patients with Cryptococcus and Aspergillus coinfection in south-western China.
Case presentation
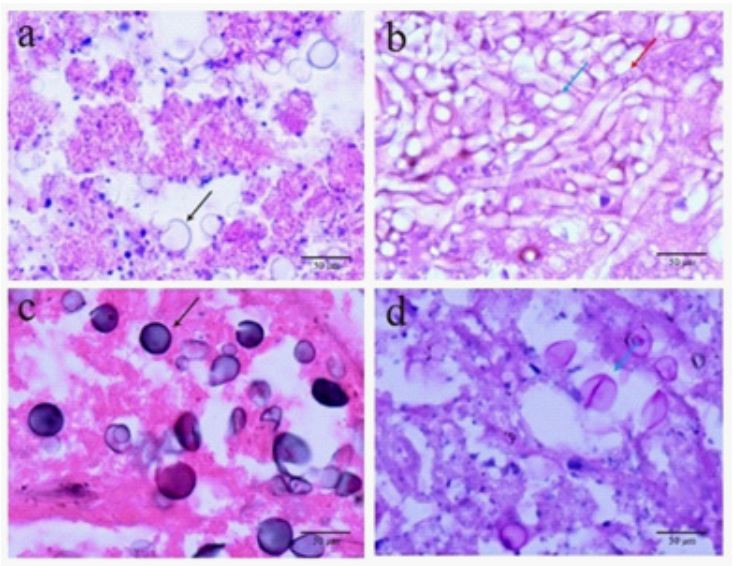
In August, 2022, a 66-year-old woman was admitted to The Medical Center Hospital of Qionglai City (Chengdu, China) with multiple pulmonary nodules. The patient appeared to be normal on physical examination. Her laboratory results showed a mild high neutrophilic granulocyte percentage of 79.6% (normal range 40-75%), a high fibrinogen concentration of 4.42 g/L (normal range 2-4 g/L), a high cancer antigen 15-3 concentration of 25.53 U/mL (normal range 0-15 U/mL) and other examination results including HIV test and hs-CRP test were negative on the day of hospital admission. She had no history of exposure to bird droppings or pollution. CT image examination of her thorax revealed an ellipsoidal low-density shadow which was considered as Lung-RADS4A level (5-15% risk about pulmonary malignancy) and a smaller solid nodule with irregular shape which was considered as Lung-RADS3 level (1-2% risk about pulmonary malignancy) in right lung on the day of hospital admission. The pulmonary function test suggested mild lung functional impairment at day +3. Next, Cryptococcus and Aspergillus were incidentally discovered by examining the pathologic tissues from lung collected by thoracoscopic surgery at day +5 and the surgery was conducted to remove those lung nodules. The diameter of Cryptococcus was 10-30 μm and Aspergillus spores were present with specific hyphal fragments like antler (Figure). The patient began to take oral fluconazole at day +5. There were a normal fungal-D-glucan concentration of 12.3 pg/mL (normal range 0-100.5 pg/mL) and negative serum cryptococcal or Aspergillus antigen results at day +12. Cerebrospinal routine and biochemical examination were normal and india ink staining was negtative at day +14. This is a patient with asymptomatic pulmonary co-infection of Cryptococcus and Aspergillus.The patient was discharged from hospital with oral fluconazole 400mg qd for half a year at day +16.
Discussion
Pulmonary Cryptococcosis (PC) and aspergillosis (PA) are caused by opportunistic infections for human via inhalation of Cryptococcus and Aspergillus spores, which have been gradually common diseases for immunocompromised patients [7,8]. The spores are inhaled into pulmonary trachea and alveoli and to activate phagocytes, in which the polysaccharide capsule that surrounds spores protects them from ingestion by phagocytes. In this way, presence and activity of spores trigger focal granulomatous inflammation in pulmonary tissue frequently [9]. Aspergillus can cause non-necrotizing granulomatous inflammation. Pneumonia caused by Cryptococcus is the early phase of cryptococcosis, which lacks diagnostic specificity. However, if it is not discovered in early phase, the asymptomatic carrier gradually occurs related symptoms with fungal infiltration, specially disseminated cryptococcosis involving brai with a poor prognosis. Cough, dyspnea and pleurisy pain are common clinical symptoms of patients that are similar to symptoms of other diseases like community-acquired pneumonia or pulmonary tuberculosis. Consequently, the diagnosis of infection is inherently more challenging. In addition, common imaging appearances of PC include solitary nodule, multiple nosules, consolidation of lobule and bronchopneumonia, and it is difficult to differentiate PC from lung cancer or bacterial pneumonia based on these appearences [10]. Generally, appearance of single pulmonary nodule is more common in non-HIV patients, and immunocompromised patients represent multiple nodules, ground-glass interstitial changes and cavitation [11,12]. In this case, the patient who was negative-HIV had a nodule caused by Cryptococcus, and another nodule caused by Aspergillus. The CT imaging of thorax was reviewed that the focus position fitting non-air distribution indicated a possible radiographic feature of Cryptococcus infection, which contributed to specificity of diagnosis. Serum Cryptococcus antigen test with high sensitivity contributes to enhance accurate diagnosis after finding of pulmonary nodule. The co-infection with the two fungus which is a unique report is rarely recorded. In brief, the infection without typical symptoms or positive laboratory reports is a challenge for clinical diagnosis.
References
- Bielska E, May RC. What makes Cryptococcus gattii a pathogen? FEMS Yeast Res. 2016; 16: fov106.
- Speed B, Dunt D. Clinical and host differences between infections with the two varieties of Cryptococcus neoformans. Clin Infect Dis. 1995; 21: 28-34.
- Rajasingham R, Smith RM, Park BJ, Jarvis JN, Govender NP, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis. 2017; 17: 873-81.
- Pappas PG, Perfect JR, Cloud GA, Larsen RA, Pankey GA, et al. Cryptococcosis in human immunodeficiency virus-negative patients in the era of effective azole therapy. Clin Infect Dis. 2001; 33: 690-9.
- Shirley RM, Baddley JW. Cryptococcal lung disease. Curr Opin Pulm Med. 2009; 15: 254-60.
- Yu JQ, Pu Tang KJ, Xu BL, Xie CM, Light RW. Pulmonary cryptococcosis in non-AIDS patients. Braz J Infect Dis. 2012; 16: 531-9.
- Chang W-C, Tzao C, Hsu H-H, Lee S-H, Huang K-L, et al. Pulmonary cryptococcosis: Comparison of clinical and radiographic characteristics in immunocompetent and immunocompromised patients. Chest. 2006; 129: 333-40.
- Liu h, Shen S, Wang Q. Recurrent pulmonary cryptococcosis during chronic HBV infection. Medicine. 2021; 100: e28250.
- Inaba A, Okada A, Yoshida T, Itoyama S, Nakai T, et al. Disseminated Cryptococcosis with Rapidly Growing Lung Nodules in an End-stage Renal Disease Patient. Intern Med. 2017; 56: 377-80.
- Hu Y, Ren SY, Xiao P, Yu FL, Liu WL. The clinical and radiological characteristics of pulmonary cryptococcosis in immunocompetent and immunocompromised patients. BMC Pulm Med. 2021; 21: 262.
- Qu J, Zhang X, Lu Y, Liu X, Lv X. Clinical analysis in immunocompetent and immunocompromised patients with pulmonary cryptococcosis in western China. Sci Rep. 2020; 10: 9387.
- Xie X, Xu B, Yu C, Chen M, Yao D, et al. Clinical analysis of pulmonary cryptococcosis in non-HIV patients in south China. Int J Clin Exp Med. 2015; 8: 3114-9.