Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
A febrile dysphagia: Clinical image
Naïke Bigé1; Nikias Colignon2; Jean-Luc Baudel1; Eric Maury1,3,4*
1Medical Intensive Care, Saint-Antoine Hospital, Paris, France.
2Department of Medical Imaging, Saint-Antoine Hospital, Paris, France.
3Pierre and Marie Curie University, Paris, France.
4INSERM, Sorbonne University, Pierre Louis Institute of Epidemiology and Public Health, Paris, France.
*Corresponding Author : Eric Maury
Medical Intensive Care, Saint-Antoine Hospital,
Paris, France.
Tel: +3301 149-28-23-18;
Email: eric.maury@aphp.fr
Received : Nov 14, 2023
Accepted : Dec 15, 2023
Published : Dec 22, 2023
Archived : www.jcimcr.org
Copyright : © Maury E (2023).
Citation: Bigé N, Colignon N, Baudel JL, Maury E. A febrile dysphagia: Clinical image. J Clin Images Med Case Rep. 2023; 4(12): 2751.
Background
A 67-year-old man was referred to ICU for hypotension, dysphagia and fever. He had received, months before, an orthotopic liver transplantation for alcoholic liver cirrhosis complicated by septic shock related to cellulitis due to Staphylococcus aureus bacteraemia. The patient was finally discharged home and did well thereafter. On admission, blood pressure was 143/64 mmHg, pulse was 96 per minute. Respiratory rate was per minute. Temperature was 38,4°C. Food ingestion initially alleviated epigastric pain but became rapidly impossible. Mottling was noted on both knees. Physical examination revealed localized abdominal tenderness. Laboratory work up and electrocardiogram were unremarkable.
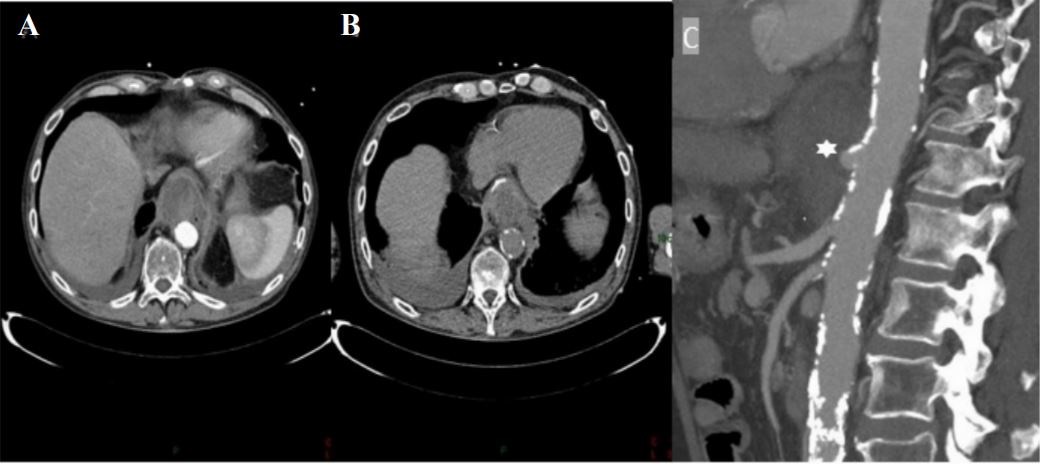
An abdominal CT scan disclosed a round-shaped mass not enhanced by intravenous contrast media located between the stomach and the aorta (Figure 1A). Barium ingestion revealed that the stomach was completely compressed by the mass (Figure 1B). Multiplanar reconstruction disclosed an aortic aneurysm developed above coeliac artery (Figure 1C). Operative findings revealed a pre-ruptured mycotic aneurysm. Blood cultures obtained on admission and operative sampling found the Staphylococcus aureus strain isolated 4 months before.