
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Extraskeletal Ewings sarcoma of the right inguinal region
Taylor Loon*, MBBCh; Amr Wardeh, MD; Ravi Adhikary, MD
SUNY Upstate Medical University, Syracuse, NY, USA.
*Corresponding Author : Taylor Loon
SUNY Upstate Medical University, Syracuse, NY,
USA.
Email: loont@upstate.edu
Received : Nov 25, 2023
Accepted : Dec 21, 2023
Published : Dec 28, 2023
Archived : www.jcimcr.org
Copyright : © Loon T (2023).
Citation: Loon T, Wardeh A, Adhikary R. Extraskeletal Ewings sarcoma of the right inguinal region. J Clin Images Med Case Rep. 2023; 4(12): 2763.
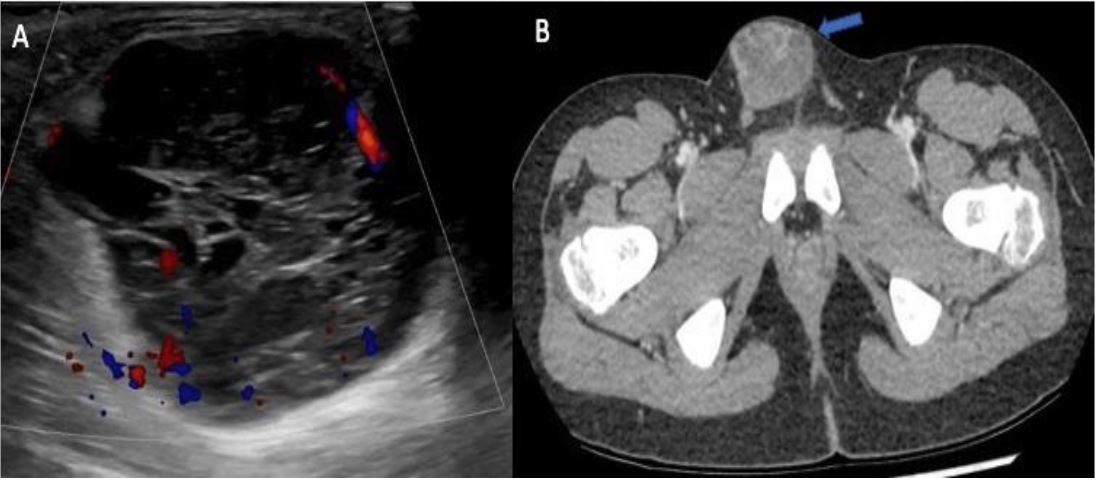
Case presentation
12-year-old Caucasian male presented to the emergency department with a two-day history of vomiting and a new rapidly growing right groin mass. The patient denied pain or urinary symptoms. Physical examination revealed a palpable, non-tender, non-reducible, semi-solid mass in the right inguinal region. Ultrasound examination showed a heterogeneous mass with solid and cystic components. CT imaging confirmed the mass is separate from the spermatic cord and the absence of lymphadenopathy.
An ultrasound-guided core biopsy was performed. Microscopic examination, immunohistochemical staining and FISH analysis confirmed a diagnosis of Extraskeletal Ewing Sarcoma (EES). Staging fluorodeoxyglucose F-18 PET/CT showed increased avidity of the mass without metastatic disease. Chemotherapy with vincristine, doxorubicin, and cyclophosphamide followed by ifosfamide and etoposide was initiated. Three months later, the patient underwent surgical resection with no recurrence or metastasis on follow-up imaging.
Discussion
EES is a rare type of Ewing Sarcoma (ES), accounting for about 25% of all cases [1]. Its average age of diagnosis is 20 years with equal gender distribution [2]. Caucasians are predominantly affected, and the most common location is the paravertebral region (30%), followed by the lower extremities (25%) [3]. EES usually presents as a rapidly growing solitary mass, with lungs and bone being metastatic sites [3].
CT is often the first imaging modality used, showing a welldemarcated mass with muscle-like density and heterogeneous enhancement [3]. MRI is the preferred method for characterizing EES, with the mass often containing areas of high T2-weighted signal intensity due to cystic change or necrosis [3]. FDG PET/ CT is sensitive for staging and detecting nodal and distant metastases, as EES typically exhibits increased metabolic activity. Definitive diagnosis requires biopsy and pathological examination.
Local disease management starts with neoadjuvant chemotherapy before radiation or surgical resection. The 5-year survival rate for localized disease is approximately 75% with appropriate chemotherapy regimens, but drops to 15-32% for metastatic disease [3].
References
- Abboud A, Masrouha K, Saliba M, et al. Extraskeletal Ewing sarcoma: Diagnosis, management and prognosis. Oncol Lett 2021; 21: 354.
- Kennedy JG, Eustace S, Caulfield R, et al. Extraskeletal Ewing’s Sarcoma: A Case Report and Review of the Literature. Spine 2000; 25: 1996.
- Wright A, Desai M, Bolan CW, et al. Extraskeletal Ewing Sarcoma from Head to Toe: Multimodality Imaging Review. Radiographics 2022; 42: 1145–60.