
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
An unusual course of rituximab
Ajibade Adenitan; Somanshi Sehgal; Aman Kumar; Lakita Gupta*; Thomas Sheeran
Department of Rheumatology, Royal Wolverhampton NHS Trust, Wolverhampton, UK.
*Corresponding Author : Lakita Gupta
Department of Rheumatology, Royal Wolverhampton NHS Trust, Wolverhampton, UK.
Email: l.gupta2@nhs.net
Received : Dec 06, 2023
Accepted : Jan 01, 2024
Published : Jan 08, 2024
Archived : www.jcimcr.org
Copyright : © Gupta L (2024).
Keywords: Rituximab; Spleen; Microinfarcts.
Citation: Adenitan A, Sehgal S, Kumar A, Gupta L, Sheeran T. An unusual course of rituximab. J Clin Images Med Case Rep. 2024; 5(1): 2783.
Description
Rituximab (RTX) is increasingly used to manage autoimmune diseases and haematological malignancies [1,2]. Contrary to the common adverse effect of hypersensitivity reactions and infection, late-onset complications of rituximab are rarely reported.
We report the case of a 36-year-old woman diagnosed with Mixed Connective Tissue Disease (MCTD) who complained of severe left-sided upper abdominal pain during a second dose of rituximab infusion. She reported a similar pain episode, albeit less extreme, during the first rituximab infusion a fortnight ago.
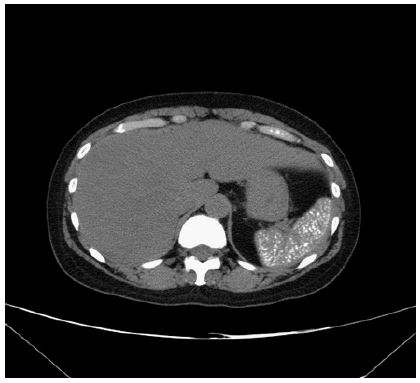
She was blue-lighted to the emergency department, where global rebound tenderness and guarding of the left upper quadrant were observed. The differentials included splenic infarction due to RTX-induced thrombosis, infection, and splenic rupture. However, abdominal CT was normal despite high inflammatory markers and neutropenia. No pathogen was identified over scans or culture. The patient improved with empiric treatment, and further doses of RTX were deferred. A repeat CT scan 12 months later showed multiple punctate calcifications studding the spleen (Figure 1), suggesting the possibility of microthrombosis/microinfarcts.
In a patient with MCTD, vasculopathy on a background of inflammation may predispose to thrombosis. RTX binds to CD20-positive B cells and plasma cells and may cause the release of antibodies and cytokines [2]. Post-RTX reactions and thrombosis have been anecdotally reported, and clinicians should be aware of it and discuss this possibility with patients having underlying vasculopathy and active inflammation such as MCTD [3].
Ethics and consent: This report adheres to Helsinki Declaration.
Conflict of interest: None.
References
- Pescovitz MD. Rituximab, an Anti-CD20 Monoclonal Antibody: History and Mechanism of Action. American Journal of Transplantation. 2006; 6: 859-66.
- Cerny T, Borisch B, Introna M, Johnson P, Rose AL. Mechanism of action of rituximab. Anticancer Drugs. 2002; 13.
- Tun NT, Mi K, Smith J. Unusual Course of Splenic Marginal Zone Lymphoma. World J Oncol. 2013; 4: 205-9.