
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Rhinoscleroma: Hard tumefaction of respiratory mucosa- A clinical picture
Marlapudi Sudheer Kumar1*; Deepthi Sangineedi1; Roohie Singh2; Sanjay Kumar3; Abhishek Singh4; Angshuman Dutta5
1Department of ENT-HNS, Resident, Command Hospital Air Force, Bangalore, India.
2Department of ENT-HNS, Professor, Command Hospital Eastern Command, Kolkata, India.
3Department of ENT-HNS, Associate Professor, Command Hospital Air Force, Bangalore, India.
4Department of Pathology, Assistant Professor, Command Hospital Air Force, Bangalore, India.
5Department of ENT-HNS, Professor and Head, Command Hospital Air Force, Bangalore, India.
*Corresponding Author : Marlapudi SK
Resident, Department of ENT-HNS, Command Hospital Air Force, Bangalore, India.
Tel: +91-8121525345;
Email: sudheerjoel.medico@gmail.com
Received : Jan 26, 2024
Accepted : Feb 13, 2024
Published : Feb 20, 2024
Archived : www.jcimcr.org
Copyright : © Marlapudi SK (2024).
Abstract
Keywords: Granulomatous disease; Hebra nose; Klebsiella; Mikulicz cells; Rhinoscleroma; Russell bodies.
Citation: Marlapudi SK, Sangineedi D, Singh R, Kumar S, Singh A, et al. Rhinoscleroma: Hard tumefaction of respiratory mucosa- A clinical picture. J Clin Images Med Case Rep. 2024; 5(2): 2870.
Description
A 34-years male, presented with left-sided nasal obstruction with mucoid nasal discharge for 3 months duration. On examination, there was a deviated nasal septum towards the right with a reddish fleshy mass in the left nasal cavity. There was decreased fogging on the cold spatula test on the left side and Cottles test was negative. This nasal mass was seen occupying the posterior choana on posterior rhinoscopy.
Diagnostic nasal endoscopy confirmed a reddish fleshy mass in left nasal cavity arising from inferior turbinate, extending along the nasal floor and impinging onto the lateral nasal wall (Figure 1a). It was sensitive to probing and bled. The probe could be passed all around the mass except the superolateral aspect where it was attached to the Inferior turbinate.
CE-MRI of Face and Paranasal sinuses showed a well-defined lobulated mass epicentered in the left nasal cavity involving the inferior turbinate. It caused expansion of the left nasal cavity and indentation on the medial wall of the left maxillary sinus (Figure 1b).
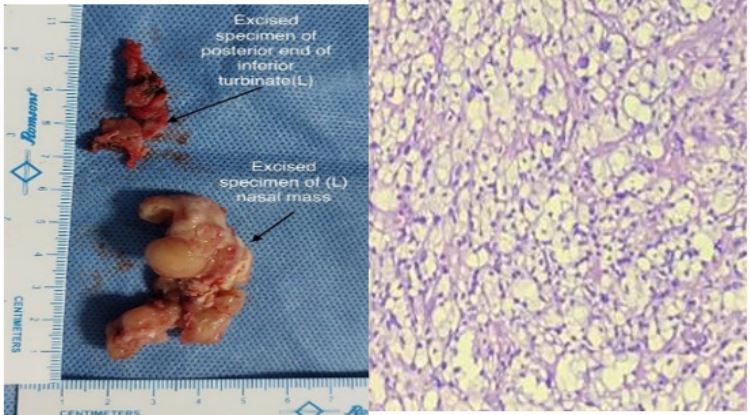
The patient underwent Endoscopic excision of the mass along with excision of the posterior part of left inferior turbinate (Figure 2a) since intraoperatively, the mass was seen to be arising from posterior part of inferior turbinate.
Histopathology revealed focally lined respiratory epithelium & sub-epithelium which showed large sheets of foamy histiocytes (Miculickz cells) containing numerous Frisch bacilli, numerous plasma cells (some with Russell bodies) and lymphocytes suggestive of Rhinoscleroma (Figure 2b). Special staining like CD68 was positive, Gram stain showed thick short plump gram-negative bacilli morphologically resembling Klebsiella. The patient recovered well after the surgery and was started on Tab Rifampicin 300 mg BD and Tab Doxycycline 100 mg OD for 06 weeks. There were no signs of recurrence during a follow up of 06 months.
Rhinoscleroma is a chronic granulomatous, slowly progressive infectious disease caused by Klebsiella rhinoscleromatis, a rod‑shaped Gram‑negative bacillus. Rhinoscleroma most commonly involves the sino-nasal cavity extending eventually into the lower airways. Rhinoscleroma progress in Three clinicopathological stages (i) the Catarrhal/Rhinitis stage, (ii) the Hypertrophic/granulomatous/florid stage, and (iii) the sclerotic/ cicatricial stage. Histopathology defines the definitive diagnosis based on characteristic Mikulicz cells and Russel bodies, as described in 1877 by Johann Von Mikulicz [1]. Intra-cytoplasmic bacilli are demonstrated using Periodic Acid-Schiff (PAS), Geimsa, Gram, silver, or Warthin-Starry stains.
Bactericidal antibiotics in large doses are given for at least four to six weeks. Recent reports support oral therapy with Tab Rifampicin, Sulphamethoxazole-Trimethoprim combination, and ciprofloxacin [2]. Local application of 2% Acriflavin for eight weeks was reported to be efficacious and non-toxic. Severe nasal obstruction and nasal deformity are common indications for surgical management. Regular follow-up is vital as clinical remission and relapse are common findings in Rhinoscleroma reaching up to 25% in 10 years [3].

References
- Simons ME, Granato L, Oliveira RC, Alcantara MP. Rhinoscleroma: case report. Braz J Otorhinolaryngol. 2006; 72(4): 568-571. doi:10.1016/s1808-8694(15)31006-5.
- Bakhiet, A., Abd Hakeem, A., Saleh, E., Sherif, M., Mohammed, A. Safety and Efficacy of Rifampicin in treatment of Rhinoscleroma, Single Institutional Experience on patients over two years period. Egyptian Journal of Neck Surgery and Otorhinolaryngology. 2021; 7(2): 23-36. doi: 10.21608/ejnso.2021.201081.
- Gaafar HA, Gaafar AH, Nour YA. Rhinoscleroma: an updated experience through the last 10 years. Acta Otolaryngol. 2011; 131(4): 440-6. doi: 10.3109/00016489.2010.539264. Epub 2011 Jan 3. PMID: 21198342.