
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Estimation of some biochemical parameters of COVID-19 patients as mortality markers: A retrospective study
Svetlana Rogacheva1,2*; Marina Barulina1,3,4; Mikhail Gromov1; Anton Reshetnikov5; Alla Fomina1
1Saratov Medical University “Reaviz”, Saratov, 410012, Russia.
2Saratov State Medical University Named After V.I. Razumovsky, Saratov, 410012, Russia.
3Perm State University, Perm, 614068, Russia.
4Institute of Precision Mechanics and Control, Russian Academy of Sciences, Saratov, 410028, Russia.
5Saratov Regional Infectious Diseases Clinical Hospital Named After N.R. Ivanov, Saratov, 410041, Russia.
*Corresponding Author : Svetlana Rogacheva
Saratov Medical University “Reaviz”, Saratov,
410012, Russia.
Email: smro13@yandex.ru
Received : Jan 08, 2024
Accepted : Feb 27, 2024
Published : Mar 05, 2024
Archived : www.jcimcr.org
Copyright : © Rogacheva S (2024).
Abstract
Aims and objective: The novel COVID-19 virus infection is known to be a multisystem disease. Moderate and severe forms of COVID-19 are usually accompanied by damage to the lungs and blood vessels, but the heart, kidneys, liver, intestines, and pancreas can also be affected. Many biochemical parameters have been shown to become altered in COVID-19 patients in correlation with the disease severity and outcome. The aim of the study was to evaluate the significance of some biochemical parameters of blood characterizing kidneys and liver functioning as markers of mortality risk in patients with COVID-19, depending on their gender and age.
Material and methods: A cohort, retrospective, cross-sectional study was conducted, which analyzed the clinical data of 195 hospital patients with a confirmed diagnosis of COVID-19 and pneumonia. The cohort was divided into groups by gender and age category. Biochemical parameters characterizing kidneys and liver functioning were analyzed: aspartate aminotransferases, alanine aminotransferases, total bilirubin, conjugated bilirubin, glucose, creatinine, urea. For correlation and statistical analysis, visualization of the results, the python language was used. The significance of differences in the parameters when comparing patient groups was assessed using one-way ANOVA and Student’s t-test.
Results: The COVID-19 mortality rate was shown to increase with the age of patients. Among the patients over 50 years of age, the women mortality was 2.3 times lower than that of men. For the entire cohort, the mortality was determined to mostly correlate with the level of creatinine (correlation coefficient Kc=0.21) and urea (Kc=0.16). Analysis by age group showed that for patients older than 65 years an increase in creatinine by 2.5 times and urea by 2.2 times relative to the norm was associated with the 100 % mortality. Analysis by gender group indicated that the poor outcome of men is most associated with the increase of age (Kc=0.34), creatinine (Kc=0.27), urea (Kc=0.27); the similar correlations were not observed in women.
Conclusion: It was found that an increase in creatinine level in COVID-19, indicating kidney damage, is more typical for men than for women (p=0.002). Creatinine >287 µmol/l and urea >18.3 mmol/l are the markers associated with the risk of COVID-19 related death in men over 65 years of age.
Keywords: Biochemical parameters of blood; COVID-19 pneumonia; Mathematical analysis; Mortality markers; Retrospective data.
Citation: Rogacheva S, Barulina M, Gromov M, Reshetnikov A, Fomina A. Estimation of some biochemical parameters of COVID-19 patients as mortality markers: A retrospective study. J Clin Images Med Case Rep. 2024; 5(3): 2900.
Introduction
At present, the mechanism of the SARS-CoV-2 virus interaction with cells and the stages of the development of the COVID-19 infectious process are well studied and described [1,4]. The presence of the SARS-CoV-2 receptor – angiotensin-converting enzyme 2 – in the cells of different tissues determines a variety of clinical manifestations of the disease [4]. The COVID-19 disease may have mild, moderate or severe symptoms, or go asymptomatically; in many cases patients have pneumonia [5]. In severe cases COVID-19 leads to pulmonary compromise and diffuse alveolar damage, causing respiratory distress and fibrosis. Some authors point to the possibility of damage to the liver, kidneys, heart and intestines in addition to lung injury due to the presence of systemic inflammation and subsequent multi-organ dysfunction [6-8]. Recent studies have shown that different laboratory parameters become altered in these patients, that is why they are useful as biomarkers to assess the progression of the disease, determine the targets of virus impact, choose therapies and predict outcome of the disease [4,9].
Several biomarkers were shown as predictors of the poor COVID-19 outcome: interleukin-6, ferritin, lactate dehydrogenase, C-Reactive Protein (CRP), procalcitonin, lymphocyte count, neutrophil to lymphocyte ratio, lymphocyte to CRP ratio, platelet count, and specific cardiac biomarkers [4]. The most of them are the markers of escalating inflammation process which is the main reason of Acute Lung Injury (ALI) and mortality in COVID-19.
A typical feature of ALI is co-localization of thrombosis and inflammation within the pulmonary capillary vasculature. Thromboinflammation causes the formation of fibrin-rich thrombi in the alveolar capillaries [10]. The process of fibrinolysis leads to the production of D-dimers which spill into the blood. Thus, Ddimer is considered to be a biomarker of coagulative cascade taking place in severe COVID-19. A level of >2.0 µg/mL on admission was shown to predict mortality [11,12]. Earlier we have shown that an increase in the D-dimer concentration by more than 625 ng/mL in patients over 80 years of age correlates with a fatal outcome [13].
The cardiac pathology is of special interest in COVID-19. In order to assess heart damage in COVID-19, it was proposed to use specific cardiac biomarkers: creatinine kinase muscle brain, cardiac troponin I, myoglobin, and N-terminal of the prohormone brain natriuretic peptide [4]. High levels of these biomarkers correlated with lethality [14,15] but their limit values for predicting mortality were lower than those for common heart disease [16].
Several studies support the idea that kidney damage is common in COVID-19 patients [6,7,17]. The proportion of Acute Kidney Injury (AKI) among complications caused by COVID-19 is estimated at 4% [8]. The studies of kidney functioning in COVID-19 patients showed that non-survivors had a progressive increase of serum creatinine and urea levels above the reference range, reaching a peak a few days before they died. Therefore, these parameters are proposed to evaluate the prognosis of patients [9].
The inflammation mediated by the immune system and/or the pharmacological treatment used during the hospitalization of patients can also have contributed to the liver injury. According to the study results [18] patients with abnormal hepatic tests (Aspartate Aminotransferases (ASAT), Alanine AminoTransferases (ALAT), bilirubin) on admission were more likely to evolve toward a serious illness.
In the previous study [13], we analyzed a significant array of physiological and biochemical indices in patients with COVID-19 pneumonia (209 people) and revealed several parameters predicting a poor outcome of the disease, namely the presence of cardiovascular diseases, oxygen saturation below 80% for patients over 50 years, D-dimer blood level 2.5 times exceeding the upper limiting value of the reference range for patients over 80 years of age.
The aim of this study was to evaluate the significance of some biochemical parameters of blood characterizing kidneys and liver functioning as markers of mortality risk in patients with COVID-19, depending on their gender and age.
Methods
There was conducted a cohort, retrospective, cross-sectional study of patients with a confirmed diagnosis of COVID-19 pneumonia hospitalized in the fall of 2020. Inclusion in the cohort was made by the criteria: 1) diagnosis of COVID-19 based on the detection of SARS-CoV-2 Ribonucleic Acids (RNA) from nasopharyngeal swabs; 2) diagnosis of pneumonia based on the chest Xray or CT images; 3) hospitalization in the V.I. Razumovsky Saratov Clinical Hospital No 2 in the fall 2020. The patients received treatment in accordance with the temporary recommendations of the Ministry of Health of the Russian Federation. The random cohort consisted of 195 patients. The studies were carried out in compliance with international and Russian ethical principles and standards, and were approved by the Ethics Committee at the Medical University “Reaviz.”
We used some data of biochemical blood test of patients fulfilled immediately after their hospitalization: ASAT, ALAT, total bilirubin, conjugated bilirubin, glucose, creatinine, urea.
For a mathematical analysis, patients were divided into five age categories: 1-18<35; 2-35<50; 3-50<65; 4-65<80; and 5- ≥ 80 years of age. The values of biochemical parameters were compared with normal reference values (Table 1) and were divided into categories relative to their reference ranges: the values corresponding to the interval of the norm were taken as 0, deviations to the greater or lesser side from the limiting values of the norm by 10, 20, 30%, etc. were written as 10, 20, 30…, with a plus or minus sign, respectively.
Correlation and scatter diagrams, matrices of pairwise correlation coefficients were plotted with the help of algorithms programmed in python using the numpy and pandas libraries (https://numpy.org/, https://pandas.pydata.org/pandas-docs/ stable/). The results were visualized using the seaborn and mathplotlib libraries (http://seaborn.pydata.org/, https://matplotlib.org/).
The significance of differences in the parameters when comparing patient groups was assessed using one-way ANOVA and Student’s t-test. The difference was considered statistically significant at the probability level p<0.05 [19].
Results and discussion
In the fall of 2020, in Saratov (Russia), there was a significant increase in the incidence of COVID-19, patients with a confirmed diagnosis, moderate or severe symptoms of COVID-19 were placed in specialized hospitals. During hospitalization, the physiological, hematological and biochemical parameters of patients were subject to mandatory registration. This study examined the records of 195 patients with COVID-19 to determine the significance of certain biochemical markers as predictors of mortality.
The studied cohort consisted of 106 women and 89 men. Nearly 53% of patients were over 65 years of age. 39 People (20% patients) deceased, of which 12.3% were men (24 people) and 7.7% women (15 people). In Table 2 we can see that the mortality rate among the patients increased with their age. In the first age group there were no fatal outcomes; in the oldest group the lethality reached 52.38% in males, 23,08% in females. Among the patients over 50 years of age, there were almost 1.5 times more women than men, whilst the mortality among women was 2.3 times lower than that among men. Our results approve the data of the other authors determined an old age and male sex as poor outcome risk factors in COVID-19 [20-22].
Table 1: Analyzed biochemical markers and their normal reference values.
| No | Biochemical parameters of blood | Designation | Reference values for | |
|---|---|---|---|---|
| Men | Women | |||
| 1. | Aspartate aminotransferases (U/L) | ASAT | 0-45 | 0-31 |
| 2. | Alanine aminotransferases (U/L) | ALAT | 0-45 | 0-31 |
| 3. | Bilirubin, total (μmol/L) | Bil_tot | 3.5-21 | 3.5-21 |
| 4. | Bilirubin, conjugated (μmol/L) | Bil_con | 0-5 | 0-5 |
| 5. | Glucose (mmol/L) | Glucose | 3.3-5.5 | 3.3-5.5 |
| 6. | Creatinine (μmol/L) | Creatinine | 62-115 | 53-97 |
| 7. | Urea (mmol/L) | Urea | 2.5-8.3 | 2.5-8.3 |
Table 2: Distribution of non-survivors by age and sex.
|
Age group |
Number of patients |
Fatal outcomes in each age
category of patients, % |
Fatal outcomes across the entire cohort, % |
||
|---|---|---|---|---|---|
| men | women | men | women | ||
| 18<35 | 22 | 0 | 0 | 0 | 0 |
| 35<50 | 33 | 13.79 | 11.89 | 1.54 | 0.51 |
| 50<65 | 37 | 26.32 | 17.59 | 2.05 | 2.05 |
| 65<80 | 58 | 33.78 | 12.12 | 3.59 | 2.05 |
| ≥80 | 45 | 52.38 | 23.08 | 5.13 | 3.08 |
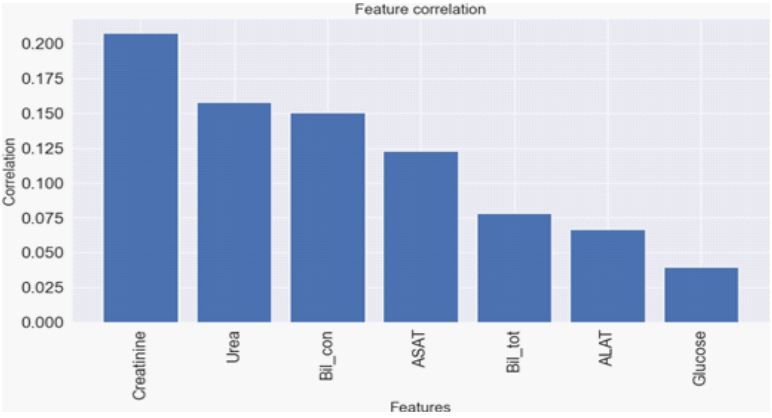
A diagram of the correlation between some biochemical parameters of patients (195 people) and a poor outcome of the disease was plotted (Figure 1). We have chosen biomarkers characterizing kidneys and liver functioning (creatinine, urea, total bilirubin, conjugated bilirubin, ASAT, ALAT, glucose).
The diagram shows that the disease mortality mostly correlates with the level of creatinine (correlation coefficient Kc=0.21). To a lesser extent, it is associated with the level of urea (Kc=0.16), direct bilirubin (Kc=0.15) and ASAT (Kc=0.125). It should be noted that correlation coefficients below 0.2 indicate the absence of a significant relationship between parameters. Previously, in a similar way, we found a high correlation of mortality from COVID-19 with the level of oxygen saturation (Kc=-0.43) and respiratory rate (Kc=0.39) of patients [13]; these markers are known to be among the eight predictors of the prognostic model of the fatal outcome in COVID-19 [20]. In a systematic review [22] high ASAT and creatinine increase were named among 35 variables that can provide valuable prognostic information on COVID-19 outcome. Bertsimas et al. [23] studied the data of 3,062 COVID-19 patients and determined blood urea nitrogen (>18 mg/dL), and blood creatinine (>1.2 mg/dL) as lethality risk factors along with decreased oxygen saturation and elevated levels of C-reactive protein.
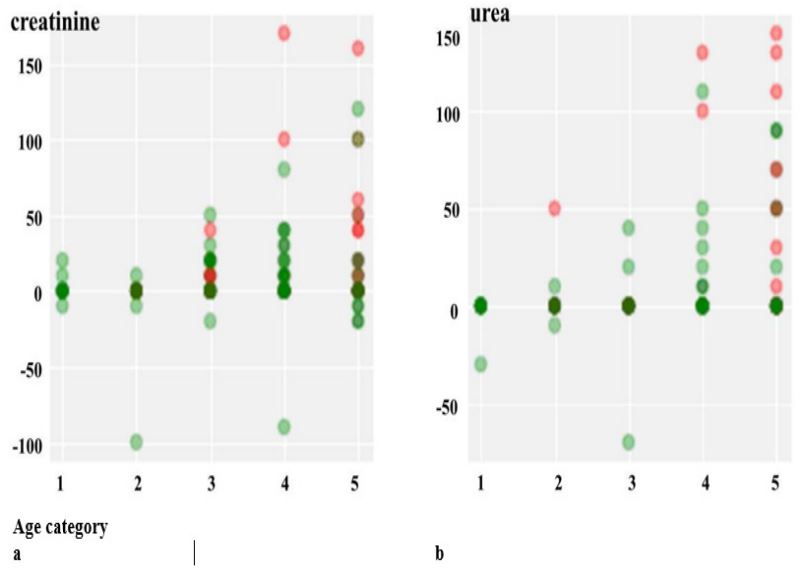
An increase in the level of serum creatinine and urea of patients with COVID-19 indicates kidney damage [6,7]. It was of interest to find out how the change in these biomarkers correlates with the mortality of patients from different age groups. For this purpose, scatter plots were built (Figure 2).
Statistical analysis was performed to identify differences in creatinine and urea levels between survivors and non-survivors from each age group (Tables 3 and 4). Table 3 shows, that the means of creatinine concentration of non-survivors of the 3-d, 4th, 5th age categories are higher than the corresponding values in survivors, but no significant differences were found between these values, apparently due to the large scatter of values. There are no significant differences in urea level between survivors and non-survivors of each age group as well (Table 4). Similar results were obtained in a retrospective study conducted on 183 COVID-19 patients [24].
Our results may indicate that kidney damage in COVID-19 is not the main, but a possible cause of death in patients, mostly older. For such patients (over 65 years of age), creatinine and urea at concentrations 2.5 and 2.2 times higher than normal, respectively, can be considered markers of lethality.
The findings are consistent with other studies that show a significant association between kidney dysfunction and the risk of AKI or death associated with COVID-19 [17,25]. There are some differences in the assessment of the incidence of AKI in patients with COVID-19. Zahid et al. [26] analyzed clinical data from 469 COVID-19 patients and identified 27.3% cases of inhospital AKI with 71.1% mortality. Moledina et al. [27] reported on 30.6% of AKI incidents among 2,600 SARS-CoV-2 positive hospitalized patients. Meta-analysis of the results of five studies, comprising 964 COVID-19 positive patients, showed that the cumulative event rate of AKI was 7.1% (95% confidence interval: 1.8%-24.5%, p<0.001, I2=92.4) [28].
It is known that the main criterion for AKI and its stages is the amount by which the serum creatinine level increases in 48 hours [29]. In the proposed classification/staging system [29] the criterion for stage 3 AKI, requiring renal replacement therapy, is the value of serum creatinine ≥354 μmol/L. This value is much higher than the survival limit of older patients we have found (287 μmol/L). Thus, in COVID-19, the threshold value of creatinine as a marker of mortality seems much lower than in the stage 3 of AKI. Undoubtedly, our results require verification on a larger number of patients.
It was of interest to find out whether there are differences in the biochemical markers of deceased and surviving patients of different gender. To do this, we plotted matrices of pairwise correlation coefficients separately using the data of male and female patients (Figure 3). Matrices, in addition to the studied biochemical parameters, include age and the poor result of the disease (Result). The more the coefficient approaches 1, the stronger the relationship between the variables. Pair correlation coefficients below 0.2 indicate the absence of a significant relationship between the parameters. To visualize the results, the color effect was used: the brighter the color, the stronger the dependence of the parameters on each other. Each figure has a color scale.
Table 3: Impact of creatinine concentration, as determined in patients of different ages at the time of hospital admission, on the disease outcome.
|
Age group |
Survivors | Non-survivors | p | ||||
|---|---|---|---|---|---|---|---|
| Number of patients |
Mean Creatinine± S, μmol/L |
Median Creatinine, μmol/L |
Number of patients |
Mean Creatinine± S, μmol/L |
Median Creatinine, μmol/L |
||
| 18 < 35 | 22 | 87.4±16.68 | 84.5 | 0 | 0 | 0 | - |
| 35 < 50 | 29 | 96.5±53.56 | 90.6 | 4 | 88.3±18.30 | 83.9 | 0.56 |
| 50 < 65 | 29 | 90.9±26.54 | 89.8 | 8 | 103.3±28.61 | 103.5 | 0.30 |
| 65 < 80 | 47 | 96.6±30.64 | 91.3 | 11 | 117.2±72.58 | 90.0 | 0.38 |
| ≥ 80 | 29 | 103.5±42.96 | 100.4 | 16 | 131.7±61.52 | 123.8 | 0.12 |
Table 4: Impact of urea concentration, as determined in patients of different ages at the time of hospital admission, on the disease outcome.
|
Age group |
Survivors | Non-survivors | p | ||||
|---|---|---|---|---|---|---|---|
| Number of patients |
Mean Urea± S, mmol/L |
Median Urea, mmol/L |
Number of patients |
Mean Urea± S, mmol/L |
Median Urea, mmol/L |
||
| 18 < 35 | 22 | 3.8±1.17 | 3.9 | 0 | 0 | 0 | - |
| 35 < 50 | 29 | 5.2±3.18 | 4.53 | 4 | 5.8±4.32 | 3.8 | 0.79 |
| 50 < 65 | 29 | 5.9±2.28 | 5.5 | 8 | 5.7±1.26 | 5.9 | 0.79 |
| 65 < 80 | 47 | 6.3±2.71 | 6.2 | 11 | 6.6±5.27 | 4.6 | 0.82 |
| ≥ 80 | 29 | 7.8±3.73 | 6.9 | 16 | 8.9±5.55 | 5.7 | 0.48 |
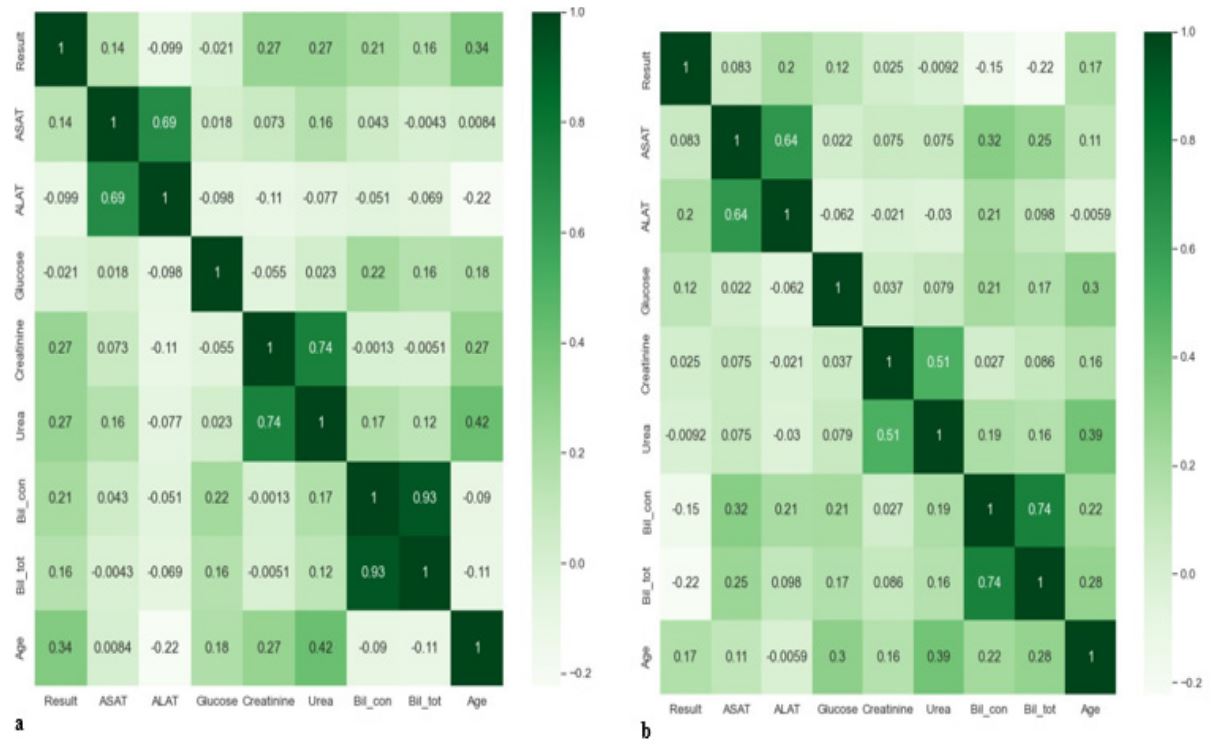
Firstly, the matrices allow us to see the interdependent biochemical markers: ALAT and ASAT (Kc=0.69 for men; Kc=0.64 for women); creatinine and urea (Kc=0.74 for men; Kc=0.51 for women); total bilirubin and conjugated bilirubin (Kc=0.93 for men; Kc=0.74 for women). It is noteworthy that the correlation coefficients of these indicators in the male sample (Figure 3a) are higher than in the female sample (Figure 3b)
Secondly, the matrices make it possible to detect indicators that are most correlated with the age of patients: in men (Figure 3a) these are urea (Kc=0.42) and creatinine (Kc=0.27), in women (Figure 3b) – urea (Kc=0.39), glucose (Kc=0.3), total bilirubin (Kc=0.28).
Table 5: Assessment of the significance of differences between values of urea and creatinine in patient groups.
| Patient groups |
Significance of differences
in biomarkers, р |
|
|---|---|---|
| Urea | Creatinine | |
| Men and women | 0.228 | 0.002 |
| Surviving men and women | 0.959 | 0.066 |
| Non-surviving men and women | 0.141 | 0.036 |
| Surviving and non-surviving women | 0.933 | 0.796 |
| Surviving and non-surviving men | 0.056 | 0.011 |
Thirdly, using the matrices, it was found that the lethal outcome of men is most associated with age (Kc=0.34), creatinine (Kc=0.27), urea (Kc=0.27), and conjugated bilirubin (Kc=0.21) (Figure 4a). In women, this relationship is not observed; there is a weak correlation of lethal outcome with the level of ASAT (Kc=0.20) and there is practically no correlation of poor outcome with age (Kc=0.17) (Figure 4b). Thus, the division of data by gender of patients allowed us to identify some differences in the course of COVID-19 pneumonia in men and women. It was noted that an increase in creatinine and urea levels, indicating kidney damage, is more typical for men than for women and is associated with the advanced age of patients.
Statistical analysis was performed to identify differences in these biomarkers between groups, differing in gender and outcome of the disease (Table 5).
Table 5 shows that there are significant differences (p<0.05) in creatinine level in patients from the groups: men and women; non-surviving men and women; surviving and non-surviving men. A rather high significance of differences (p=0.056) in the content of blood urea of surviving and non-surviving men was found. Thus, the totality of the obtained results allows us to propose blood biomarkers creatinine (>287 μmol/L) and urea (>18.3 mmol/L) as predictors of COVID-19 mortality only for men over 65 years of age. These biochemical markers were not predictive for women. It should be noted that Oussalah et al. [17] determined the significance of urea nitrogen >0.42 g/L as a marker associated with the risk of COVID-19 related death, this value is equal to 14.28 mmol/L urea, which is very close to our result. Cheng et al. [25] assessed serum creatinine level >133 μmol/L as a risk factor of in-hospital death from COVID-19, that does not contradict the results of our study.
The weak correlation of the lethal outcomes of men with the level of conjugated bilirubin, women – with the level of ASAT, which we found, can be considered as confirmation of the published data that patients with abnormal liver tests (ASAT, ALAT, bilirubin) were more likely to progress towards serious disease [18]. Thus, changes in these biomarkers in patients with COVID-19 also require the attention of physicians.
Conclusion
COVID-19 is a new viral disease with different clinical manifestations. In severe cases COVID-19 leads not only to lung injury, but also to dysfunction of the other organs, such as the liver, kidneys, heart and intestines. Biomarkers play a crucial role in early diagnosis, recognition of complications, management of patients, predicting the outcome of the disease.
Using a mathematical analysis of retrospective data from 195 patients with COVID-19 pneumonia, we evaluated some biochemical parameters of blood (ASAT, ALAT, bilirubin total and conjugated, glucose, creatinine, urea) as predictors of the disease mortality depending on the age and gender of patients.
Weak correlations of increasing creatinine and urea levels with patient mortality were found. When comparing the male and female cohorts, it was noted that these indicators are associated only with male mortality (Kc=0.27). Analysis by age group determined that creatinine >287 µmol/L and urea >18.3 mmol/L can be considered markers of mortality risk in men over 65 years of age. Thus, kidney damage in COVID-19 is one of the causes of death, and the development of such a process is most likely for older men. These biomarkers might support to identify high mortality risk cases in the initial admission phase.
Declaration of interest: All the authors declare that they have no conflict of interest in this work.
Funding: This study was conducted without external financial support.
References
- Hoffmann M, Kleine-Weber H, Schroeder S, Kru N, Erichsen S, Schiergens TS, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020; 181(2): 271-280. https://doi.org/10.1016/j.cell.2020.02.052.
- Mishra SK and Tripathi T. One year update on the COVID-19 pandemic: where are we now? Acta Tropica. 2021; 214: Article 10577. https://doi.org/10.1016/j.actatropica.2020.105778.
- Ou X, Liu Y, Lei X, Li P, Mi D, Ren L, et al. Characterisation of spike glycoprotein of SARS-CoV-2 on virus entry and its immune crossreactivity with SARS-CoV-2. Version 2. Nature Communications. 2020; 11(1): 1620. https://doi.org/10.1038/s41467-020-15562-9.
- Samprathi M and Jayashree M. Biomarkers in COVID-19: an upto-date review. Frontiers in Pediatrics. 2021; 8: 607647. https://doi.org/10.3389/fped.2020.607647.
- Dong X, Cao Y-Y, Lu X-X, Zhang J-J, Du H, Yan Y-Q, et al. Eleven faces of coronavirus disease. Allergy. 2020; 75(7): 1699-1709. https://doi.org/10.1111/all.14289.
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020; 395: 507-513. https://doi.org/10.1016/S0140-6736(20)30211-7.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395: 497-506. https://doi.org/10.1016/S0140-6736(20)30183-5.
- Wu T, Zuo Z, Kang S, Jiang L, Luo X, Xia Z, et al. Multi-organ dysfunction in patients with COVID-19: A systematic review and meta-analysis. Aging and Disease. 2020; 11(4): 874-894. http://dx.doi.org/10.14336/AD.2020.0520.
- Letelier P, Encina N, Morales P, Riffo A, Silva H, Riquelme I. and Guzmán N. Role of biochemical markers in the monitoring of COVID-19 patients. J Med Biochem. 2021; 40(2): 115-128. https://doi.org/10.5937/jomb0-29341.
- Mitchell WB. Thromboinflammation in COVID-19 acute lung injury. Paediatric Respiratory Reviews. 2020; 35: 20-24. https://doi.org/10.1016/j.prrv.2020.06.004.
- Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z and Zhang Z. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J Thromb Haemost. 2020; 18(6): 1324-1329. https://doi.org/10.1111/jth.14859.
- Yao Y, Cao J, Wang Q, Shi Q, Liu K, Luo Z, et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study. Journal of Intensive Care. 2020; 8: 49. https://doi.org/10.1186/s40560-020-00466-z.
- Gromov MS, Rogacheva SM, Barulina MA, Reshetnikov AA, Prokhozhev DA and Fomina AYu. Analysis of some physiological and biochemical indices in patients with COVID-19 pneumonia using mathematical methods. Journal of Evolutionary Biochemistry and Physiology. 2021; 57(6): 1394-1407. https://doi.org/10.1134/S0022093021060181.
- Li JW, Han TW, Woodward M, Anderson CS, Zhou H, Chen YD and Neal B. The impact of 2019 novel coronavirus on heart injury: a systematic review and meta-analysis. Progress in Cardiovascular Diseases. 2020; 63: 518-24. https://doi.org/10.1016/j.pcad.2020.04.008.
- Deng P, Ke Z, Ying B, Qiao B and Yuan L. The diagnostic and prognostic role of myocardial injury biomarkers in hospitalized patients with COVID-19. Clinica Chimica Acta. 2020; 510: 186-90. https://doi.org/10.1016/j.cca.2020.07.018.
- Qin J-J, Cheng X, Zhou F, Lei F, Akolkar G, Cai J, et al. Redefining cardiac biomarkers in predicting mortality of inpatients with COVID-19. Hypertension. 2020; 76: 1104-12. https://doi.org/10.1161/HYPERTENSIONAHA.120.15528.
- Oussalah A, Gleye S, Urmes IC, Laugel E, Barbe F, Orlowski S, et al. The spectrum of biochemical alterations associated with organ dysfunction and inflammatory status and their association with disease outcomes in severe COVID-19: a longitudinal cohort and time-series design study. EclinicalMedicine. 2020; 27: 100554. https://doi.org/10.1016/j.eclinm.2020.100554.
- Cai Q, Huang D, Yu H, Zhu Z, Xia Z, Su Y, et al. COVID-19: abnormal liver function tests. Journal of Hepatology. 2020; 73(3): 566-574. https://doi.org/10.1016/j.jhep.2020.04.006.
- Greenwood PE, and Nikulin MS. A guide to chi-squared testing. New York. John Wiley & Sons. 1996.
- Knight SR, Ho A, Pius R, Buchan I, Carson G, Drake TM, et al. Risk stratification of patients admitted to hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4C Mortality Score. BMJ. 2020; 370: 3339. https://doi.org/10.1136/bmj.m3339.
- Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. Journal of Infection. 2020; 81(2): 16-25. https://doi.org/10.1016/j.jinf.2020.04.021.
- Izcovich A, Ragusa MA, Tortosa F, Lavena Marzio MA, Agnoletti C, Bengolea A, et al. Prognostic factors for severity and mortality in patients infected with COVID-19: a systematic review. PLoS ONE. 2020; 15(11): 0241955. https://doi.org/10.1371/journal.pone.0241955.
- Bertsimas D, Lukin G, Mingardi L, Nohadani O, Orfanoudaki A, Stellato B, et al. COVID-19 mortality risk assessment: an international multi-center study. PLoS ONE. 2020; 15(12): 0243262. https://doi.org/10.1371/journal.pone.0243262.
- Mir SM, Tahamtan A, Nikoo HR, Arabi MS, Moradi AW, Ardakanian S and Tabarraei A. Evaluation of biochemical characteristics of 183 COVID-19 patients: a retrospective study. Gene Reports. 2022; 26: 101448. https://doi.org/10.1016/j.genrep.2021.101448.
- Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney International. 2020; 97: 829-38. https://doi.org/10.1016/j.kint.2020.03.005.
- Zahid U, Ramachandran P, Spitalewitz S, Alasadi L, Chakraborti A, Azhar M, et al. Acute Kidney Injury in COVID-19 patients: an innercity hospital experience and policy implications. American Journal of Nephrology. 2020; 51: 786-796. https://doi.org/10.1159/000511160.
- Moledina DG, Simonov M, Yamamoto Y, Alausa J, Arora T, Biswas A, et al. The association of COVID-19 with acute kidney injury independent of severity of illness: a multicenter cohort study. American Journal of Kidney Diseases. 2021; 77(4): 490-499. https://doi.org/10.1053/j.ajkd.2020.12.007
- Lotfi B, Mohammadrahimi M, Hajebrahimi S, Kabiri N, Vahed N, Jahantabi E, et al. COVID-19 outbreak and the impact on renal disorders: a rapid review. Turkish Journal of Urology. 2020; 46(4): 253-261. https://doi.org/10.5152/tud.2020.20179
- Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG and Levin A. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Critical Care. 2007; 11: Article R31. https://doi.org/10.1186/cc5713.