
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case report of endovascular treatment of a fast-growing inflammatory abdominal aortic aneurysm in a patient with Staphylococcus aureus sepsis
Madara Bruvere1; Patricija Ivanova1,2,3*; Veronika Zaiceva2; Aina Kratovska2,3; Sanita Ponomarjova2,4; Signe Zelca4,5; Vitalijs Zvirgzdins1
1Department of Vascular Surgery, Riga Eastern Clinical University Hospital, Riga, Latvia.
2Department of Interventional Radiology, Riga East Clinical University Hospital, Riga, Latvia.
3Faculty of Medicine, University of Latvia, Riga, Latvia.
4Riga Stradins University, Riga, Latvia.
5Department of Internal Diseases, Riga East Clinical University Hospital, Riga, Latvia.
*Corresponding Author : Patricija Ivanova
Department of Vascular Surgery, Riga Eastern Clinical University Hospital, Latvia.
Email: patricijaivanova@gmail.com
Received : Feb 26, 2024
Accepted : Mar 20, 2024
Published : Mar 27, 2024
Archived : www.jcimcr.org
Copyright : © Ivanova P (2024).
Abstract
Abdominal Aortic Aneurysm (AAA) and its subsequent rupture is one of the life-threatening conditions. The most common type of arterial aneurysm, AAA, becomes significant at a diameter greater than 3 cm. The mean growth rate of an AAA is 2-3 mm per year, and surgical repair is usually recommended if the diameter exceeds 5.5 cm, in men and 5.0 to 5.2 cm, in women. Faster-growing aneurysms are more aggressive and have a greater risk of rupture. We report a case of a 64-year-old, comorbid male patient who was found to have a previously unknown, but a rapidly growing AAA, which grew from 6cm to 8 cm within just 3 weeks. He was admitted in the emergency department with complaints of worsening dyspnea even without exertion. Upon thorough diagnostic tests, the severity of the overall medical condition was determined by S. aureus sepsis, decompensation of cardiovascular disease, and secondary kidney injury due to septic shock. While receiving treatment for sepsis, a diagnostic CT imaging was done, which confirmed bilateral pneumonia and retroperitoneal abscess in m. psoas major mass, and an infrarenal abdominal aortic aneurysm, which was 6cm in diameter at the time of diagnosis. Another control CT of the lungs and abdomen was performed three weeks later, indicating the pneumonia was slowly resolving, while the aortic aneurysm increased in dynamic; the diameter was 8 cm with a penetrating exudation on the left side, m. psoas abscess was still observed, but decreasing. Because the AAA was very fast-growing, it greatly increased the risk of its rupture, therefore a decision was made to perform endovascular abdominal aortic aneurysm repair, despite the risk of stent infection, given the patients septic background. The goal of this case report is to highlight the rare case of a rapidly growing inflammatory aneurysm and its successful endovascular management. While it’s known that 5-10% of all AAA are inflammatory, cases of surgical treatment in the setting of sepsis are basically non-existent in the literature [1].
Keywords: Intra-ocular pressure; Glaucoma.
Citation: Bruvere M, Ivanova P, Zaiceva V, Kratovska A, Ponomarjova S, et al. A case report of endovascular treatment of a fast-growing inflammatory abdominal aortic aneurysm in a patient with Staphylococcus aureus sepsis J Clin Images Med Case Rep. 2024; 5(3): 2948.
Introduction
Abdominal Aortic Aneurysm (AAA) and its subsequent rupture still have a significant mortality rate. The mean growth rate of an AAA is usually 2-3 mm per year [2]. Aneurysm repair is usually recommended if the anterior to posterior size exceeds 5.5 cm, in men and 5.0 to 5.2 cm, in women; while faster-growing aneurysms are more aggressive and present a greater risk [3]. While it’s known that inflammatory aneurysms compromise 5-10% of all cases, reports of their surgical treatment in the setting of sepsis are close to non-existent [1]. Treatment of inflammatory aneurysms presents a great dilemma because of associated peri-aortic inflammation, increasing the risk of intraoperative injury to anatomical structures.
Case presentation
A 64-year-old male patient was admitted in the emergency department with complaints of worsening dyspnea and shortness of breath even without exertion. His medical history was remarkable for known cardiovascular disease, including coronary artery disease with previous myocardial infarction, hypertensive cardiomyopathy, chronic heart disease NYHA III, primary arterial hypertension of secondary degree. He regularly takes the following medications for the management of his cardiovascular diseases: Aspirin, Nebivolol, Ramipril, Atorvastatin, Torsemide and Spironolactone. Other comorbidities included chronic obstructive pulmonary disease, treated with Fenoterol inhalation, pulmonary hypertension, adiposity of third degree, managed with Atorvastatin, psoriasis, and polyarthritis. On presentation, the patients’ vital signs were stable, verbal contact was possible, but with disturbed consciousness. Results of his physical examination included bilateral rhonchi and crackles on lung auscultation; a regular heart rate and rhythm; and an enlarged abdomen that was soft and not painful to palpation.
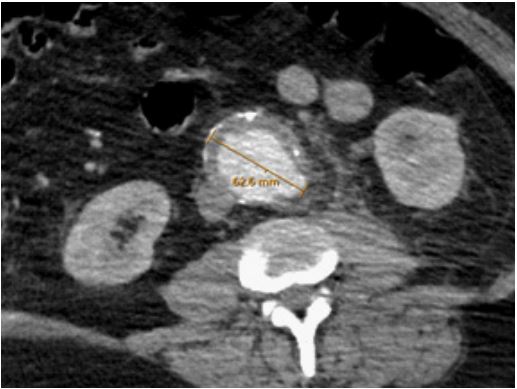
Laboratory results were remarkable for infection, acute kidney injury, and heart failure (CRP 335 mg/L, creatinine 398 micromole/ L, GFR 14 ml/min, leukocytes 38.88x109 /L) neutrophils 36.41x109 /L, D-dimers 5.59/mL, T-troponin 73 ng/L, proBNP 16360 pg/mL. CT imaging was done, which confirmed bilateral pneumonia, but more importantly, an infrarenal abdominal aortic aneurysm, which was 6cm in diameter at the time of diagnosis; 06.07.2022 (Figure 1).
The severity of the patient’s overall medical condition was determined by sepsis, decompensation of cardiovascular disease, and secondary kidney injury due to sepsis. On the evening of admission, the patient was admitted to the sepsis unit, where due to an increasing potassium level (7.7 mmol/L) and decreasing diuresis, the decision to start renal replacement therapy was made. Because of increasing psychomotor restlessness and respiratory failure, the patient was intubated, and MVP was started. The following days, septic shock developed and vasopressor support with Noradrenaline and Adrenaline was initiated. Moreover, S. aureus bacteremia and bacteriuria was detected, so a diagnosis of S. aureus sepsis was established. Because of intensive therapeutic measures, the patient’s overall condition started to improve after about 2 weeks. As diuresis recovered and renal parameters improved, RRT was stopped. Inflammatory markers also decreased, hemodynamic stability was restored, consequently vasopressor therapy was withdrawn, and the patient was extubated. Another CTA of the lungs and abdomen was performed 3 weeks after the initial CT was made, indicating the pneumonia was slowly resolving, while the aortic manifestations increased in dynamic; the AAA was now 8 cm with a penetrating exudation on the left side, m. psoas abscess was still observed, but decreasing (Figure 2).

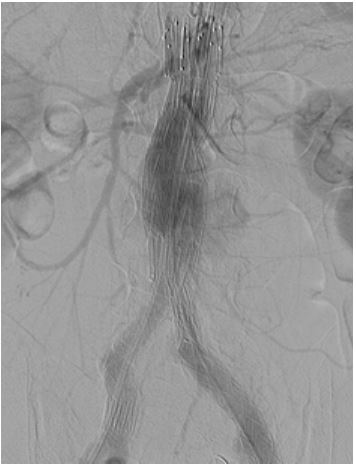
Because the AAA was very fast-growing, it greatly increased the risk of its rupture. Open surgery was contraindicated, given that the patient had evidence of infection and abscedation in the retroperitoneal m. psoas region and due to his overall severe condition carried out high risk for surgery. A decision was made to perform endovascular abdominal aortic aneurysm repair, despite the risk of stent infection, given the patients septic background. Endovascular repair was done with a standard ZenithFlex (COOK) stent graft system (Figure 3). Postoperatively, the patient received targeted intravenous antibacterial therapy with Ceftriaxone, Erythromycin, Metronidazole and Piperacillin/ Tazobactam. Postoperative period was without complications and the patient was discharged in an objectively good condition with detailed recommendations on the 10th postoperative day, for further outpatient treatment under the supervision of a general practitioner.
A follow-up CT angiography was done one year after the endovascular therapy (Figure 4).
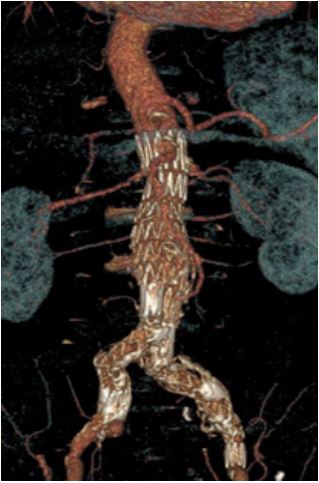
The patient has been under close monitoring with his GP, as well as a team of vascular surgeons and interventional radiologists. As seen in on the CT angiography scan, the placed stent graft type does not have a significant Type II endoleak, no enlargement of the aneurysmal sac, and no signs of infection.
Discussion
Our case highlights the possible connection between abdominal aortal aneurysm growth rate and inflammation and sepsis. In the past, AAA has been looked at as a chronic process because of long-term atherosclerotic lesion development, but recent studies suggest that inflammatory processes, oxidative stress, intraluminal thrombus formation, and extracellular matrix degeneration play an equally important role, because they contribute to the growth rate of the aneurysm [5]. Inflammatory cells are known to secrete proteases, enzymes, that cause destruction of the Extracellular Matrix (ECM) and its subsequent degradation. Because the backbone of the blood vessel is destroyed, the tunica media loses its resistance and elasticity, furthermore, inflammatory cells can accumulate in the media layer, resulting in inflammatory cell infiltration into the media [6]. This, together with platelet accumulation and activation of the coagulation cascade, contribute to intraluminal thrombus formation, which causes dilation of the aorta even more, and predisposes it to rupture.
This patient had an asymptomatic AAA, and it was an incidental finding, whilst looking for an acute infectious process causing his septic condition. If the aneurysmal size would have stayed the same, its repair could have been delayed until the patient recovered and was fit for surgery, but considering its rapid growth rate of 2 cm in practically 3 weeks, we had to follow emergent indications, and repair it right away to prevent its rupture.
Infections account for about 2% of AAAs and can be divided into 4 types: post- traumatic infected false aneurysms, mycotic aneurysms, microbial arteritis, and infection of an existing aneurysm. The latter has a 90% mortality rate [7]. The consensus among vascular surgeons is that all infected aneurysms should be treated as surgical emergencies, regardless of the shape and size, but the diagnosis remains quite challenging. The universal rule is to always consider a mycotic aneurysm, when rapid expansion on serial CT scans is observed. The most significant clue that led us to the right diagnosis and rapidly initiated treatment was the rapid change in the character of the AAA. This case demonstrates a successful emergent endovascular treatment of a fast-growing inflammatory aneurysm with high risk of an endograft infection, with no signs of infection in 1 year follow up.
References
- Hellmann DB, Grand DJ, Freischlag JA. Inflammatory abdominal aortic aneurysm. JAMA. 2007; 297(4): 395-400. doi: 10.1001/jama.297.4.395. PMID: 17244836.
- Moll, FL, et al. “Management of Abdominal Aortic Aneurysms Clinical Practice Guidelines of the European Society for Vascular Surgery.” European Journal of Vascular and Endovascular Surgery : the Official Journal of the European Society for Vascular Surgery, U.S. National Library of Medicine. 2012. https://pubmed.ncbi.nlm.nih.gov/21215940/.
- Swerdlow, Nicholas J., et al. “Open and Endovascular Management of Aortic Aneurysms.” AHA Journals. 2019. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.118.313186.
- Shuai, Tao, et al. “High-Risk Factors Related to the Occurrence and Development of Abdominal Aortic Aneurysm.” Journal of Interventional Medicine, Elsevier. 2020. https://www.sciencedirect.com/science/article/pii/S2096360220300223.
- Sakalihasan N, Michel JB, Katsargyris A, Kuivaniemi H, Defraigne JO, Nchimi A, Powell JT, Yoshimura K, Hultgren R, “Abdominal Aortic Aneurysms.” Nature Reviews. Disease Primers, U.S. National Library of Medicine. 2018. https://pubmed.ncbi.nlm.nih.gov/30337540/.
- “Antithrombotic Therapy in Abdominal Aortic Aneurysm: Beneficial or Detrimental?” Blood, U.S. National Library of Medicine. 2018. https://pubmed.ncbi.nlm.nih.gov/30228233/.
- Alonso M, Caeiro S, Cachaldora J, Segura R. Infected abdominal aortic aneurysm: in situ replacement with cryopreserved arterial homograft. J Cardiovasc Surg. 1997; 38: 371-5.