
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Rhabdomyolysis: A lesser-known complication of hyperosmolar hyperglycemic coma
Karabulut Korin*; Upadhyay Ashish
Department of Medicine, Nephrology Division, Boston University Chobanian & Avedisian School of Medicine, USA.
*Corresponding Author : Korin K
Department of Medicine, Nephrology Division, Boston University Chobanian & Avedisian School of Medicine, USA.
Email: korin.karabulut@gmail.com
Received : Mar 15, 2024
Accepted : Apr 05, 2024
Published : Apr 12, 2024
Archived : www.jcimcr.org
Copyright : © Korin K (2024).
Abstract
Hyperglycemic Hyperosmolar State (HHS) is a severe complication of diabetes mellitus. Here we present a 57-year-old male with no known past medical history, who complained of polyuria, lethargy, and fever. On admission, he was found to have HHS and Acute Kidney Injury (AKI). Despite correction of hyperglycemia with insulin infusion and prompt fluid resuscitation, AKI initially worsened, which prompted thorough workup. Further workup revealed severe rhabdomyolysis. AKI is common in HHS, presumably due to hypovolemia. However, severe hyperglycemia may also contribute to rhabdomyolysis and worsen kidney injury. As other causes for rhabdomyolysis were ruled out, HHS was felt to be the most likely etiology of patient’s rhabdomyolysis.
Keywords: Rhabdomyolysis; Hyperosmolar hyperglycemic coma; Diabetic ketoacidosis; Acute kidney injury.
Citation: Korin K, Ashish U. Rhabdomyolysis: A lesser-known complication of hyperosmolar hyperglycemic coma. J Clin Images Med Case Rep. 2024; 5(4): 2984.
Introduction
Hyperglycemic Hyperosmolar State (HHS) is a life-threatening complication of diabetes mellitus, characterized by severe hyperglycemia and lack of ketoacidosis. Acute kidney injury is common amongst patients with HHS, presumably due to hypovolemia given osmotic diuresis, and it is generally reversible with intravenous fluid resuscitation. However, few case reports have been published, suggesting that hyperglycemic emergencies can contribute to the development of rhabdomyolysis, further aggravating acute kidney injury and causing higher morbidity and mortality [1]. Although the pathophysiology is unclear, it is posited that hyperosmolar state may elevate intracellular calcium, which may activate neutral proteases and lead to muscle membrane damage [2]. In addition, electrogenic sodium pump is inhibited by hyperosmolarity leading to a fall in transmembrane potential and myocyte cell wall damage [3]. Electrolyte imbalances, such as hypokalemia and hypophosphatemia associated with HHS, can play a role in rhabdomyolysis in these patients. Here, we present a 57-year-old male with no known medical history who was found to have acute kidney injury in the setting of HHS-associated rhabdomyolysis.
Case presentation
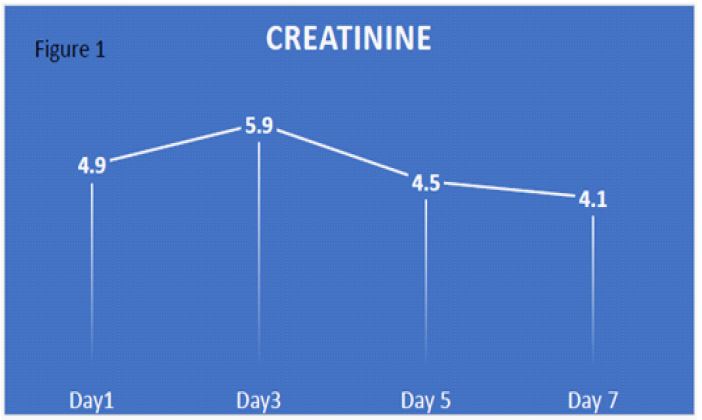
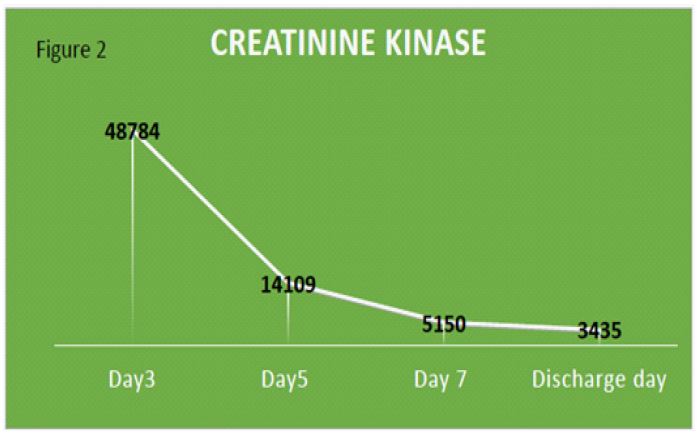
57-year-old man with no known past medical history, presented with polyuria and lethargy, and was found to be in HHS with newly diagnosed diabetes mellitus. Physical examination was mostly unrevealing, except for dry oral mucosa, lethargy, high body mass index, and fever (101.5° Fahrenheit). Initial laboratory tests showed hyperglycemia (serum glucose: 1069 mg/dL), hyperosmolarity (serum osmolality: 415 mosm/kg H2O), trace positive urine ketone, creatinine of 4.9 mg/dl (with last creatinine of 1.35 mg/dL, six years before presentation), blood urea nitrogen of 76 mg/dl, hypernatremia (167 mmol/L). In the light of the initial clinical state and diagnostic test results, he was admitted to the intensive care unit with a working diagnosis of HHS and AKI. Patient was started on aggressive intravenous fluid replacement and insulin infusion (0.1 IU/kg/h). As the patient had a mild fever, extensive infectious work-up was done, including lumbar puncture, blood culture, urine culture and abdominal ultrasound, and results were all unremarkable. With prompt treatment, his electrolyte imbalance started to improve except for the kidney function which continued to deteriorate. Urine sediment microscopy revealed muddy brown casts, no dysmorphic cells, or cellular casts. Renal sonogram showed normal sized kidneys, without any echogenicity or hydronephrosis. Thyroid function tests were within normal limits. Toxicology tests for cocaine, amphetamine and toxic alcohols were negative. Patient denied taking any prescription or over the counter medications or supplements. On hospital day 3, although the patient did not have an initial presentation to suspect rhabdomyolysis, serum creatinine kinase was checked. He was found to have rhabdomyolysis with significantly high levels of serum Creatine Phosphokinase (CPK) (48,784 U/L, reference range: 39-193 U/L).
After the patient was found to have profound rhabdomyolysis, aggressive fluid resuscitation was continued. He was able to tolerate large volume resuscitation with good urine output, without any signs of significant volume overload. Serum creatinine peaked at 5.95 mg/dL on hospital day 3 and slowly went down to 3.7mg/dl on discharge (Table 1). Treatment of rhabdomyolysis is mainly intravenous fluid resuscitation, however, in some cases, renal replacement therapy may be needed. Our patient responded to intravenous fluids with improvement of serum creatinine kinase and serum creatinine levels (Figures 1 and 2). As we ruled out common causes of rhabdomyolysis, including trauma, physical exertion, extreme body temperature changes, drugs, toxins, infections, hypokalemia, hypophosphatemia and hypocalcemia, we posit that the patient’s rhabdomyolysis was associated with HHS.
Table 1: Results on day 1 and day 3.

Discussion
Hyperglycemic Hyperosmolar State (HHS) is a severe complication of diabetes mellitus. Acute Kidney Injury (AKI) is common in HHS, presumably due to hypovolemia. However, previous reports suggest that hyperosmolarity as a result of hyperglycemic emergencies may itself lead to severe muscle injury [1]. While pathophysiology has not been fully elucidated, it is posited that the hyperosmolar state may rapidly elevate intracellular calcium , activate cell proteases, disturb cell membrane integrity, and release cell products like myoglobin and CPK into the circulation [1]. In addition, hyperosmolarity may inhibit the electrogenic sodium pump, leading to a fall in transmembrane potential and myocyte cell wall damage [2,3]. Hypokalemia and hypophosphatemia associated with HHS can also contribute to rhabdomyolysis.
Less than 10% of patients with rhabdomyolysis present with a classic triad of myalgia, dark colored urine, and muscle weakness. Most patients only exhibit mild abnormal laboratory results and may remain asymptomatic. Elevated level of CPK is a sensitive indicator of muscle injury, yet the extent of CPK elevation does not consistently correlate with the severity of muscle damage or renal failure [4]. While CPK higher than 5000 international units/L indicates a significant muscle injury and provides a reasonable sensitivity and specificity for the diagnosis of rhabdomyolysis. The McMahon scoring system, which uses readily available demographic and laboratory data, is more specific than CPK alone at predicting the need for renal replacement therapy [5].
Acute Kidney Injury (AKI) is the most important systemic complication of rhabdomyolysis, occurring at an incidence ranging from 10 to 55%, and is linked with unfavorable clinical outcomes, particularly in the presence of multiple organ failure [6]. Vasoconstriction, tubular ischemia, tubular obstruction due to myoglobin precipitation, and inflammation are some of the putative mechanisms for AKI in rhabdomyolysis [6].
The primary approach to managing rhabdomyolysis is to prevent acute kidney injury and its associated complications, such as electrolyte imbalances, arrhythmias, Disseminated Intravascular Coagulation (DIC), and shock. Treatment primarily involves generous fluid resuscitation with 0.9% sodium chloride, and diuretic therapy may also be considered if the patient becomes oliguric or significantly hypervolemic. In the past, urine alkalinization with sodium bicarbonate was used to prevent heme pigment precipitation, however it is not commonly used in current practice. As, there has not been a study performed comparing outcomes with normal saline infusion and sodium bicarbonate. In addition, urine alkalinization has potential risks, such as hypocalcemia and calcium phosphate precipitation. Mannitol was considered potentially helpful, by promoting diuresis and acting as an antioxidant, however its routine use is not recommended given the lack of evidence support and also possible risks with volume depletion, hypernatremia and controversially volume expansion and hyperosmolarity when used at high doses in the setting of reduced kidney function [8].
Early initiation of renal replacement therapy was previously suggested to aid in prompt renal recovery by clearing myoglobin and averting its tubular precipitation. However, myoglobins are not readily removed by dialysis membranes and there is insufficient evidence to support this strategy [9]. Renal replacement therapy may be needed if there is severe kidney failure, but it should not be instituted to prevent or aid in kidney recovery. While not a standard treatment, limited data exists regarding the use of plasmapheresis for rhabdomyolysis. Nonetheless, there is no discernible difference in overall outcomes and mortality with plasmapheresis compared to standard care [10].
Conclusion
Hyperglycemic hyperosmolar state is an under-recognized cause of rhabdomyolysis. Thus, through this case report, we aim to raise awareness of rhabdomyolysis as a potential complication of HHS.
References
- Mercer S, Hanks L, Ashraf A. Rhabdomyolysis in Pediatric Patients With Diabetic Ketoacidosis or Hyperglycemic Hyperosmolar State: A Case Series. Glob Pediatr Health. 2016; 3: 2333794X16671391. doi: 10.1177/2333794X16671391. PMID: 28229089; PMCID: PMC5308516.
- Singhal PC, Abramovici M, Ayer S, Desroches L. Determinants of rhabdomyolysis in the diabetic state. Am J Nephrol. 1991; 11(6): 447-50. doi: 10.1159/000168357. PMID: 1819210.
- Singhal PC, Schlondorff D. Hyperosmolal state associated with rhabdomyolysis. Nephron. 1987; 47(3): 202-4. doi: 10.1159/000184492. PMID: 3683689.
- Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis -- an overview for clinicians. Crit Care. 2005; 9(2): 158-69. doi: 10.1186/cc2978. Epub 2004 Oct 20. PMID: 15774072; PMCID: PMC1175909.
- McMahon GM, Zeng X, Waikar SS. A risk prediction score for kidney failure or mortality in rhabdomyolysis. JAMA Intern Med 2013; 173(19): 1821-1828.
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009; 361(1): 62-72.
- Brown CVR, Rhee P, Chan L, et al. Preventing renal failure in patients with rhabdomyolysis: do bicarbonate and mannitol make a difference? J Trauma Inj Infect Crit Care 2004; 56: 1191-1196.
- Zeng X, Zhang L, Wu T, Fu P. Continuous renal replacement therapy (CRRT) for rhabdomyolysis. Cochrane Database Syst Rev. 2014; 6: CD008566.
- Boparai S, Lakra R, Dhaliwal L, Hansra RS, Bhuiyan MAN, Conrad SA, Krishnan P. Therapeutic Plasma Exchange in Severe Rhabdomyolysis: A Case-Control Study. Cureus. 2023; 15(5): 39748. doi: 10.7759/cureus.39748. PMID: 37398832; PMCID: PMC10310893.