
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Prenatal diagnosis of bronchogenic cyst at the lingual base: Case report
Khezami Asma1*; Grich Amenallah2; Khomsi Dorra3; Masmoudi Aida4; Douira Khomsi Wiem5
1Department of Pediatric Medical Imaging, Radiology Resident, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
2Department of Pediatric Medical Imaging, Radiology Consultant, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
3Department of Pediatric Medical Imaging, Internal Medicine Resident, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
4Department of Embryo-Foetopathology, Professor in Embryology, Maternity Center, Tunis, Tunisia.
5Chief of Pediatric Medical Imaging, Professor in Radiology, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
*Corresponding Author : Khezami Asma
Department of Pediatric Medical Imaging, Radiology Resident, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
Tel: +21 624677063;
Email: asma.khezami95@gmail.com
Received : Mar 05, 2024
Accepted : Apr 15, 2024
Published : Apr 22, 2024
Archived : www.jcimcr.org
Copyright : © Asma K (2024).
Keywords: Bronchogenic cyst; Fetal cervical cyst.
Citation: Asma K, Amenallah G, Dorra K, Aida M, Wiem DK. Prenatal diagnosis of bronchogenic cyst at the lingual base: Case report. J Clin Images Med Case Rep. 2024; 5(4): 3002.
Short report
A 39-year-old female woman with no previous history presented at 19 weeks of pregnancy for a routine fetal ultrasound. It was her third pregnancy with no notable event so far. No particular familial or personal medical history was revealed.
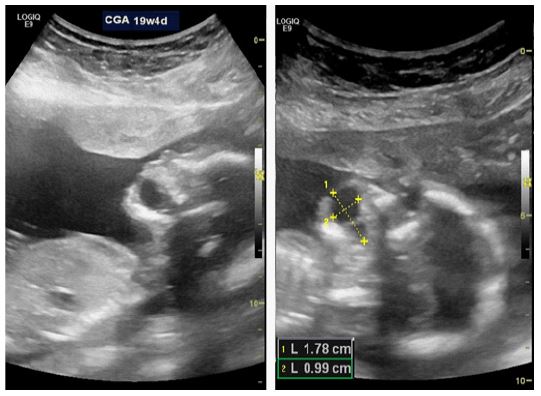
The biometry corresponded to a term of 19 weeks and 4 days gestational age of a male fetus with no major malformation except a cervical cystic mass that was discovered near the floor of the mouth. The cyst was located right on the midline, had a well-defined and thin peripheral wall with regular contours and pure anechoic material (Figure 1). It contained a single fine septum with no intrinsic signal on colour Doppler and measured 18 x 10 mm. All these findings supported a cervical lymphatic malformation, and a medical interruption of the pregnancy was proposed to the couple after interdisciplinary decision.
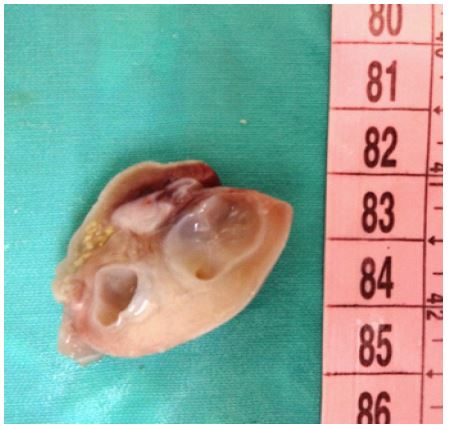
A fetal pathological examination was led with parental consent. It confirmed the diagnosis of a cystic mass at the base of the tongue (Figures 2 and 3) containing structural elements of the airways including a ciliated epithelium, and thus concluding to an extra-thoracic bronchogenic cyst.
The neck is a rare localisation of bronchogenic cysts, whereas the mediastinum and the thorax are the most frequent localisations [1,2]. We have not found many publications of similar localisations at the base of tongue through our brief literature review. Bronchogenic cysts originate from abnormal development of the primitive oesophagus and the tracheobronchial tree [3].They are generally unilocular, filled with mucus and their wall is multilayered containing components of the airways: Cartilage, smooth muscle, mucous glands and ciliated respiratory epithelium [3]. Prenatal ultrasound can easily detect a unilocular cyst located in the mediastinum, the thorax or the neck area, filled with anechoic fluid and surrounded by a well-defined thin wall [3]. However, research revealed the possibility of bronchogenic cysts presenting as hyperechoic lesions [4]. The principal threats to the fetus that can occur in cases of large cysts include heart compression and lung compression causing secondary parenchymal hypoplasia with the progressive bronchial obstruction, as reported by D. Levine et al. [5]. The evaluation of these risks has motivated the interdisciplinary decision of pregnancy interruption in our case. In the majority of cases, bronchogenic cysts are asymptomatic in the post-natal period. When they are symptomatic, they manifest through repeated bronchopulmonary infections and airway obstruction [6].

References
- Nolasco-de la Rosa AL, Nuñez-Trenado LA, Román-Guzmán E, Chávez-Villicaña CE. Neck bronchogenic cyst. Case report and review of the literature. Cir Cir Engl Ed. 1 mai. 2016; 84(3): 235‑9.
- Masson E. EM-Consulte; Kyste bronchogénique cervical chez un enfant. Available on: https://www.em-consulte.com/article/282172/kyste-bronchogenique-cervical-chez-un-enfant
- Rios LTM, Araujo Júnior E, Nardozza LMM, Moron AF, Martins M da G. Prenatal Diagnosis and Postnatal Findings of Bronchogenic Cyst. Case Rep Pulmonol. 2013; 2013: 483864.
- Iavazzo C, Eleftheriades M, Bacanu AM, Hassiakos D, Botsis D. Congenital Cystic Adenomatoid Malformation: Is There a Need for Pregnancy Termination? Case Rep Med. 2012. Available on: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3312219/.
- Levine D, Jennings R, Barnewolt C, Mehta T, Wilson J, et al. Progressive Fetal Bronchial Obstruction Caused by a Bronchogenic Cyst Diagnosed Using Prenatal MR Imaging. Am J Roentgenol. 2001; 176(1): 49‑52.
- Kaji T, Takamatsu H, Noguchi H, Tahara H, Fukushige T, et al. Cervico-Mediastinal Bronchogenic Cyst Occurring in the Prenatal Period: Report of a Case. Surg Today. 2000; 30(11): 1016‑8.