
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Ultrasound typical aspect of hypertrophic pyloric stenosis
Bouanane Rania*; Belkouchi Lina; Taibi Ouiam; Siham El Haddad; Nazik Allali; Latifa Chat
Department of Radiology, Children Hospital of Rabat, Faculty of Medicine and Pharmacy of Rabat, Morocco.
*Corresponding Author : Bouanane Rania
Department of Radiology, Children Hospital of Rabat, Faculty of Medicine and Pharmacy of Rabat, Morocco.
Tel: +21 266723547.
Email: raniabouanane@gmail.com
Received : Mar 22, 2024
Accepted : Apr 16, 2024
Published : Apr 23, 2024
Archived : www.jcimcr.org
Copyright : © Rania B (2024).
Citation: Rania B, Lina B, Ouiam T, Haddad SE, Allali N, et al. Ultrasound typical aspect of hypertrophic pyloric stenosis. J Clin Images Med Case Rep. 2024; 5(4): 3004.
Case description
A 3-week-old boy was admitted to the pediatric emergency department for vomiting and dehydration. There was no medical history records, the toddler was only breastfed and clinical signs appeared a week prior through non-bilious, projectile curdled milk emesis happening shortly after feeding, associated to clinical signs of dehydration and weight loss.
The ultrasound findings were very characteristics of HyPertrophic Pyloric Stenosis (HPS), revealing in the longitudinal view the “cervix sign”: prolonged and narrowed pyloric channel (21 mm) (yellow arrow, A), and the “Antral nipple sign” that refers to a redundant pyloric mucosa protruding into the gastric antrum (green arrow, A).
In the transverse view, “the target or donut sign” represents the hypertrophic hypoechoic muscular layer surrounding the echogenic mucosa. The pyloric muscle thickness is measured to 4 mm (red arrow, B), and the pyloric transverse diameter measures 14 mm (white arrow, B).
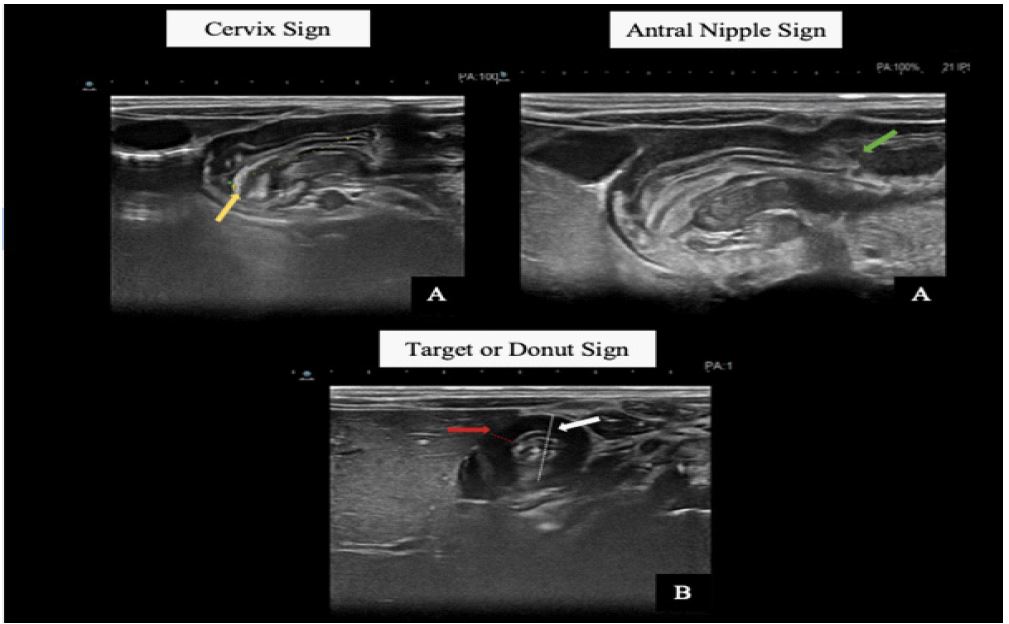
A: Longitudinal view:
Cervix sign: The length = 21 mm (yellow arrow).
Antral Nipple sign: The double layer of thickened mucosa protruding through the antrum (green arrow).
B: Transverse view:
Target or Donut sign: The muscle wall thickness = 4 mm (red arrow), and the total pyloric thickness diameter = 14 mm (white arrow).
Discussion
Hypertrophic Pyloric Stenosis (HPS) is characterized by hypertrophy and hyperplasia of the pyloric sphincter muscles, leading to the progressive obstruction of the gastric outlet [1-3]. The etiology is not fully understood, but it is believed to involve genetic, environmental, and hormonal factors. It is more common in males and first-born children.
The classic presentation includes projectile non-bilious vomiting, a palpable olive-like mass in the abdomen, and dehydration, typically manifesting between 6 to 12 weeks of age.
Muscle thickness: On a transverse image, the most reliable diagnostic criterion is a muscle wall (hypoechoic component) thickness exceeding 3 mm.
Muscle length: longitudinal length of the pyloric muscle is measured, with values over 15-17 mm indicating HPS.
Pyloric Volume: An abnormally large pyloric volume, greater than 1.5 cm³, is consistent with the diagnosis.
Pyloric diameter: A transverse diameter over 13 mm further supports the presence of HPS.
Additionally, ultrasound may demonstrate characteristic sonographic signs specific to HPS:
Antral nipple sign: In a longitudinal view, this sign is seen as a protrusion of the pyloric mucosa into the lumen of the antrum.
Cervix sign: Resembling the cervix on longitudinal view, this sign represents the elongated and narrowed pyloric channel.
Target or donut sign: A cross-sectional view that depicts the pyloric sphincter as concentric rings, resembling a target.
Retrograde peristalsis and exaggerated peristaltic waves: These are dynamic signs of peristaltic movement observed during the ultrasound, suggestive of the stomach’s effort to overcome the obstruction.
Treatment initially focuses on rehydration and electrolyte rebalance, followed by surgical treatment with pyloromyotomy. This procedure, which can be done both by laparotomy and laparoscopy, has a high success rate and low morbidity, with a recurrence rate being rare and typically indicative of an incomplete initial procedure.
References
- Marta Hernanz-Schulman et al., Infantile Hypertrophic Pyloric Stenosis. RSNA Radiology. 2003.
- Fenne AIM van den Bunder et al. Diagnostic accuracy of palpation and ultrasonography for diagnosing infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis. British Journal of Radiology. 2022.
- Samir Pandya et al., Pyloric stenosis in pediatric surgery: an evidence-based review. Surg Clin North Am. 2012.