
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pigmented eyelid hidrocystoma: A rare variant with diagnostic challenges
Elkafi Khadija*; S Chiguer; MR Bentouhami; Y Hidane; A Mchachi; L Benhmidoune; R Rachid; M Elbelhadji
Department of Adult Ophthalmology, 20 Août 1953 Hospital / IbnRochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author : Elkafi Khadija
Department of Adult Ophthalmology, 20 Août 1953 Hospital / IbnRochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Email: elkafikhadija@gmail.com
Received : Apr 05, 2024
Accepted : May 07, 2024
Published : May 14, 2024
Archived : www.jcimcr.org
Copyright : © Khadija E (2024).
Abstract
Eyelid hidrocystomas, typically benign tumors, develop from the sweat glands of the eyelids and present as skin-colored papules or nodules. The presence of pigmentation in eyelid hidrocystomas is rare and can pose a diagnostic challenge. Our study presents a case of pigmented eyelid hidrocystoma in a young woman, highlighting the importance of accurate recognition of this rare variant. We discuss the clinical, histological features, and treatment options, emphasizing the need for a differentiated approach to avoid confusion with malignant lesions.
Keywords: Hidrocystoma; Pigmented; Rare; Diagnostic challenges..
Citation: Khadija E, Chiguer S, Bentouhami MR, Hidane Y, Mchachi A, et al. Pigmented eyelid hidrocystoma: A rare variant with diagnostic challenges. J Clin Images Med Case Rep. 2024; 5(5): 3047.
Introduction
Eyelid hidrocystomas are adnexal tumors, usually benign, that develop from the eccrine or apocrine sweat glands of the eyelids. They present as skin-colored papules or nodules, often translucent, and can cause aesthetic concerns or symptoms such as itching or irritation [1]. Eyelid hidrocystomas are typically non-pigmented. However, the presence of pigmentation in these lesions is rare and can complicate their differential diagnosis.
Here, we report a case of pigmented eyelid hidrocystoma with a detailed analysis of its clinical, histological characteristics.
Case presentation
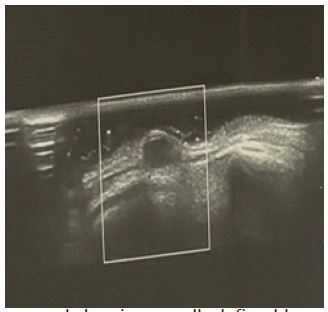
A 21-year-old woman with no significant medical history presented for the management of a lower eyelid lesion of the left eye evolving for 8 months. Examination revealed a discretely pigmented lesion, 4 mm in diameter on the left lower eyelid, without inflammatory signs or associated symptoms (Figure 1). Ocular ultrasound was performed, showing a well-defined hypoechoic oval lesion with no color Doppler signal measuring 5.4 x 2.8 mm (Figure 2).



Surgical excision of the lesion was performed, with histopathological study suggesting pigmented apocrine hidrocystoma.
Discussion
Due to the diversity of these adnexal structures, the eyelid is the site of a wide variety of benign and malignant adnexal tumors, among which hidrocystomas are found [2]. These tumors generally present in two main forms: apocrine hidrocystomas and eccrine hidrocystomas. Apocrine hidrocystomas, also known as apocrine cysts, arise from apocrine sweat glands and are often located near the eyelashes or in the eyelid fold. In contrast, eccrine hidrocystomas, or eccrine cysts, originate from eccrine sweat glands and typically present as small, translucent skin lesions, often located on the lower eyelid. Both eccrine and apocrine hidrocystomas are considered non-proliferative retention cysts [3]. They typically affect patients in their seventh decade and affect both women and men equally, except in cases of multiple cysts, where women are more affected than men [4]. Clinically, these lesions present as a papule or cystic nodule, asymptomatically dome-shaped, 1 to 4 mm in size on the lower eyelid, with a predilection for the left eye. The lesions can be flesh-colored, translucent, milky white, blue, amber, brown, or black. The reasons for the more frequent involvement of the lower eyelid and the higher incidence of cysts on the left side remain unknown [2,3]. Eccrine hidrocystomas tend to be smaller (1-6 mm in diameter) than apocrine hidrocystomas (3-15 mm in diameter). They are exacerbated by hot and humid weather conditions [5-7]. In contrast, apocrine hidrocystomas are more likely to be solitary and dark in color. They are common near the inner canthus. However, apocrine hidrocystomas are less likely to occur in the periorbital area or on body sites where apocrine glands are typically prominent [8].
Pigmented eyelid hidrocystomas are rare, with only a few cases reported in the literature. This pigmented variant can be clinically confused with pigmented vascular, epithelial, and melanocytic proliferations. Amber, brown, bluish, and even black coloration is generally attributed to lipofuscin pigments and/or its oxidation products in colloidal suspension reflecting high-energy blue wavelengths (Tyndall effect) [9-11]. Rarely, iron (hemosiderin) or melanin deposits are identified in hidrocystomas. However, the Tyndall effect, rather than specific pigments, is considered the cause of most pigmented hidrocystomas clinically [2,3]. Histologically, hidrocystomas appear as large unilocular or multilocular dermal cysts typically lined by a double layer of epithelial cells with an outer layer consisting of myoepithelial cells and an inner layer of tall columnar epithelial cells [12]. Hidrocystomas can be treated in several ways, depending on their size, number, and location. Trichloroacetic acid injection may be an option for smaller cysts. Botulinum toxin can be used to block the nerve endings of apocrine glands, thereby reducing their secretion and decreasing cyst size. Topical application of atropine, an anticholinergic agent, may also be used to reduce glandular secretion.
Electrodessication and laser therapy are other options that may be considered for the treatment of hidrocystomas. However, when hidrocystomas are pigmented or present concerning features raising suspicion of malignancy, histopathological confirmation is recommended [2-4].
Conclusion
The recognition and understanding of pigmented hidrocystomas are crucial in medical practice. These skin lesions often present subtle clinical features that can be confused with malignant tumors, such as basal cell carcinoma or melanoma. The ability to distinguish pigmented hidrocystomas from malignant lesions is essential to ensure accurate diagnosis and appropriate treatment.
References
- Agharbi FZ. Hidrocystome palpébral. Pan Afr Med J. 2019. Disponible sur: http://www.panafrican-med-journal.com/content/article/33/70/full/
- Al-Rohil RN, Meyer D, Slodkowska EA, Carlson JA. Pigmented Eyelid Cysts Revisited: Apocrine Retention Cyst Chromhidrosis. Am J Dermatopathol. Avr. 2014; 36(4): 318.
- Rosso MV, Rodriguez Kowalczuk MV, Martinez Piva MM, Mazzuoccolo LD. What could this dark lesion on a woman’s eyelid be? Int J Womens Dermatol. 24 août. 2022; 8(3): e037.
- Jakobiec FA, Zakka FR. A reappraisal of eyelid eccrine and apocrine hidrocystomas: microanatomic and immunohistochemically studies of 40 lesions. Am J Ophthalmol. Févr. 2011; 151(2): 358-374.e2.
- Sarabi K, Khachemoune A. Hidrocystomas-a brief review. MedGenMed Medscape Gen Med. 6 sept 2006; 8(3): 57.
- Talsania N, Langman G, Orpin SD. A blue nodule on the forehead. Clin Exp Dermatol. Juill. 2009; 34(5): 645-6.
- Rappazzo KC, Cohen PR. Pigmented hidrocystoma of nasal epithelium (PHONE): Report of a man with a pigmented hidrocystoma of his nose and literature review. Dermatol Online J. 15 mai. 2016; 22(5): 13030/qt9c50d26x.
- Kaur C, Sarkar R, Kanwar AJ, Mohan H. Multiple eccrine hidrocystomas. J Eur Acad Dermatol Venereol JEADV. Mai. 2002;16(3): 288-90.
- Jakobiec FA, Stacy RC, Colby KA. Pigmented apocrine hidrocystoma of the caruncle. Cornea. nov 2010;29(11):1320-2.
- Cramer HJ. [The black hidrocystoma (Monfort). Dermatol Monatschrift. Févr. 1980; 166(2): 114-8.
- Smith JD, Chernosky ME. Apocrine Hidrocystoma (Cystadenoma). Arch Dermatol. 1 mai. 1974; 109(5): 700-2.
- Zaballos P, Bañuls J, Medina C, Salsench E, Serrano P, et al. Dermoscopy of apocrine hidrocystomas: A morphological study. J Eur Acad Dermatol Venereol JEADV. Mars. 2014; 28(3): 378-81.