
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Advanced therapy of extraintestinal manifestations: A case report
Vitório Abido Neto1; Abel Botelho Quaresma2*
1Medical School Student, University of the West of Santa Catarina, UNOESC, Joaçaba, Brazil.
2Colorectal Surgery Department, University of the West of Santa Catarina, UNOESC, Joacaba, Brazil.
*Corresponding Author : Abel Botelho Quaresma
Colorectal Surgery Department, University of the West of Santa Catarina, UNOESC, Joacaba, Brazil.
Tel: +55 (49) 99914-8677;
Email: abel@proctoclinic.com.br
Received : Apr 22, 2024
Accepted : May 07, 2024
Published : May 14, 2024
Archived : www.jcimcr.org
Copyright : © Quaresma AB (2024).
Abstract
Inflammatory Bowel Disease (IBD) can trigger a variety of signs and symptoms that affect tissues adjacent to the intestine, known as Extra Intestinal Manifestations (EIM), which can significantly impact quality of life, work performance and treatment adherence. In this context, we retrospectively report the case of a patient with Ulcerative Colitis (UC), without previous success in two treatments with biological agents, treated at the University Medical Outpatient Clinic of the University of the West of Santa Catarina, simultaneously presenting four MEIs, including pyoderma gangrenous, erythema nodosum, aseptic abscess and spondyloarthritis. We describe the investigation carried out and the actions adopted by the multidisciplinary team until the clinical picture was resolved. We conclude that the approach to MEI in patients with IBD represents a challenge for health professionals, highlighting the importance of knowledge of medication possibilities and the importance of a multidisciplinary team for effective treatment.
Keywords: Extraintestinal manifestations; Inflammatory bowel disease; Biologicals; Small molecules; Ulcerative colitis.
Abreviations: ADA: Adalimumab; ABCD: Brazilian Association of Ulcerative Colitis And Crohn’s Disease; CRP: C-Reactive Protein; CD: Crohn’s Disease; EIM: Extraintestinal Manifestation; FC: Fecal Calprotectin; FPE: Fecal Parasitological Examination; GIT: Gastrointestinal Tract; IBD: Inflammatory Bowel Disease; IFX: Infliximab; NSAID: Nonsteroidal Anti-Inflammatory Drugs; RCT: Randomized Controled Trial; TOFA: Tofacitinib; TNF: Tumor Necrosis Factor; UC: Ulcerative Colitis; AMU: University Medical Outpatient Clinic; UNOESC: University of the West of Santa Catarina; UST: Ustekinumab; VEDO: Vedolizumab.
Citation: Neto VA, Quaresma AB. Advanced therapy of extraintestinal manifestations: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3049.
Introduction
Extraintestinal Manifestations (EIM) of Inflammatory Bowel Disease (IBD) consist of inflammatory processes in patients with IBD outside the Gastrointestinal Tract (GIT). They are present in more than 50% of patients with IBD and their pathogenesis is an extension/translocation of the intestinal inflammatory response, or an event perpetuated by IBD with the same genetic propensity as the underlying disease.
There are several EIMs, which can affect different tissues, however, some are the most prevalent, such as: peripheral arthritis types 1 and 2, sacroilitis, ankylosing spondylitis (osteomuscular), erythema nodosum, psoriasis and pyoderma gangrenosum (dermatological), scleritis, episcleritis and uveitis (ocular) among others in different parts of the body [1].
The most effective treatment used today for severe EIMs are corticosteroids and immunobiological drugs, such as Infliximab (IFX), Adalinumab (ADA), Ustekinumab (UST), Vedolizumab (VEDO) and Tofacitinib (TOFA) [2,14]. According to the literature, all of them can lead to clinical remission in the affected patient.
The treatment of EIM is of fundamental importance [15,16], as in addition to avoiding complications, it can improve the quality of life of patients [17], avoiding absence from work. Furthermore, there is a lack of articles in the literature that present treatment algorithms for EIM in IBD as there is controversy in the comparison between the available drugs, as well as guidance on pharmacological associations between these drugs [18]. There is also difficulty in accessing the combination of these drugs, due to the high cost and lack of coverage by public health systems, leading to judicialization [19].
The aim of this study is to discuss these difficulties by presenting the journey of a patient, suffering from UC with failure of 2 biologicals and presenting multiple EIM [20,23].
Materials and methods
The research was made based on a retrospective research in medical documents and medical records from a University Medical Outpatient Clinic of the University of the West of Santa Catarina - UNOESC, from 2018 to 2024, plus a review of the most recent literature about the treatment of the EIM of IBD.
Case report
Female patient, 27 years old, housewife, born in Curitiba - PR and resident in Herval d’Oeste - SC, comes to the University Medical Outpatient Clinic (AMU) of the University of the West of Santa Catarina (UNOESC) in April 2018 for an outpatient consultation of IBD and coloproctology. She reported that for 3 years she has had severe colicky abdominal pain, with daily diarrhea of up to 6 bowel movements per day, the presence of blood and mucus and tenesmus. She also had migratory joint pain. The patient had already been diagnosed with Crohn’s Disease (CD) since 2015, with several treatment attempts with relative improvement in symptoms. She reported significant leukopenia after using 2 months of azathioprine previously. In 2017, she consulted a specialist doctor (coloproctologist) who diagnosed UC and started using mesalazine (2 g per day) and ADA every 2 weeks without significant improvement after 8 months of use. The proctological examination was uneventful. Corticosteroids were prescribed (prednisone 40 mg/day) and the dose of mesalazine was increased to 3 g/day. ADA dose has been optimized for weekly use. This caused the condition to stabilize, with a reduction in the number of bowel movements (1 to 2 times a day), an improvement in the appearance of the feces (Bristol 5), as well as the absence of mucus and blood. Laboratory tests were requested.
At the next consultation in May 2018, she presented fecal calprotectin (FC) of 800 mg/dl, significant anemia (hematocrit 25%, hemoglobin 8.2 g/dl), negative FPE (fecal parasitological examination) and stool culture. Ferrous sulfate was introduced to treat anemia and other medications were maintained. We requested flexible rectosigmoidoscopy.
At the beginning of August of the same year, without the use of corticosteroids, she complained again of diarrhea and bleeding that had started 8 days ago. In flexible rectosigmoidecto rectosigmoidectomy, erosive retitis, Mayo 2 and biopsy with chronic and acute nonspecific inflammation without the presence of granulomas. The use of corticosteroids (prednisone 20 mg/day) was reintroduced and mesalazine was increased to 4 g/day. We opted to exchange ADA for IFX in the usual attack dose. In the following months we saw the gradual improvement of symptoms, leaving the patient in clinical remission.
In October 2020, the patient became pregnant and as the disease was in remission, the obstetrician advised the withdrawal of medications, but 60 days later she started experiencing bloody diarrhea three times a day associated with rectal pain that remained without any treatment during this period. In February 2021, the patient returned to the IBD outpatient clinic with laboratory results showing FC of 2,698 mcg/g, CRP< 6 mg/L. Once again, we opted for corticosteroid therapy (20mg/day), reintroduction of mesalazine (1.6 g/day) and the biologic that had been discontinued. We suggested not suspending the medication even close to birth, advising on vaccination after the birth of the child.
In September 2021, the patient returns to the coloproctology outpatient clinic, after a normal full-term birth, without obstetric or pediatric complications, having been referred by the health center due to abdominal pain, diarrhea, anemia, and hematochezia, 2 months ago. A colonoscopy was requested and the use of prednisone 40 mg once a day for five days was resumed, followed by 20 mg daily for ten days.
Upon return, without having had a colonoscopy, the patient reported that due to malaise, hematochezia, and intense pain, she took ibuprofen on her own. She reported, she also had arthralgia in her wrists and elbows. She said she noticed pieces of undigested mesalazine tablets in the feces. We discovered that the mesalazine supplier was changed by the state and the patient started using a generic drug produced by another laboratory. It was then recommended that a colonoscopy be carried out urgently to change treatment due to loss of response to treatment. We opted for a dose of 4.8 g/day of mesalazine and were advised to divide the medication for better absorption and the risks of using NSAIDs (Nonsteroidal anti-inflammatory drugs) in patients with UC. Due to the ineffectiveness of the treatment, we decided to prescribe mesalazine 500 mg, changing the brand we had been using (Mesalazine 800 mg, EMS®) for another (Pentasa® 500 mg), prednisone 20 mg and maintaining the IFX. Another data collected in the story was that at some point in 2021, the IFX received by the patient (Remicade® Jansen) was exchanged for a biosimilar (Rensima® Celltrion). Without knowing what led to the recurrence: changing the mesalazine generic, changing the biological product or even the loss of response that often occurs during treatment, we opted to optimize IFX with the use of 10 mg/kg (Rensima® Celltrion).
Thirty days later, the condition was still present, but with no significant laboratory changes and a colonoscopy with the diagnosis of left-sided colitis suggestive of UC Mayo 3. After 12 weeks of treatment (February 2022) we did not see any significant improvement when IFX was replaced by VDZ at the usual dose. Due to bureaucratic problems, the patient only received the first dose of VDZ at the end of December 2022, being administered in January 2023.
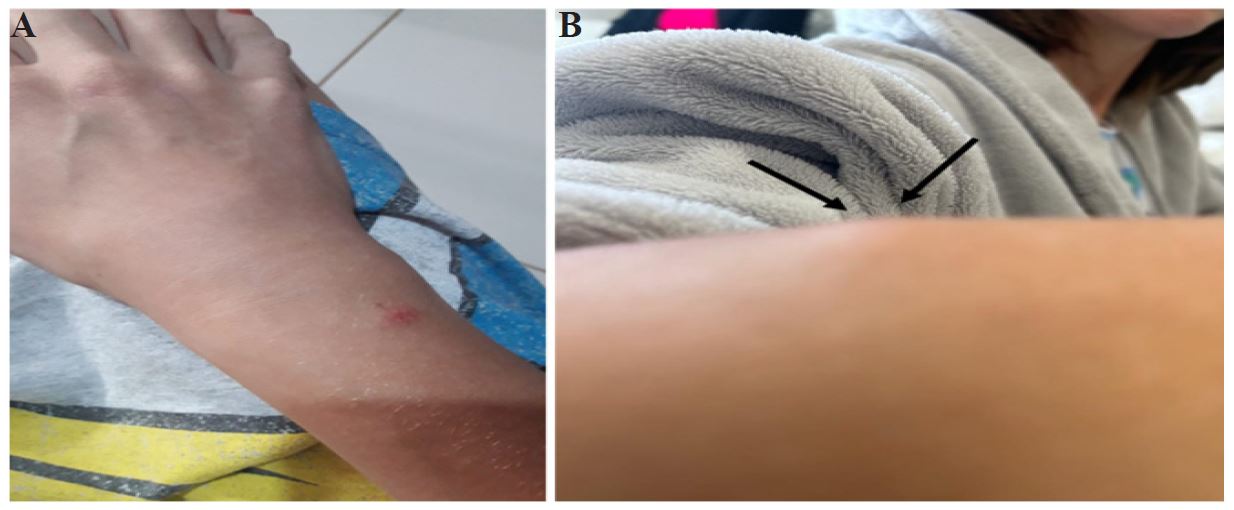
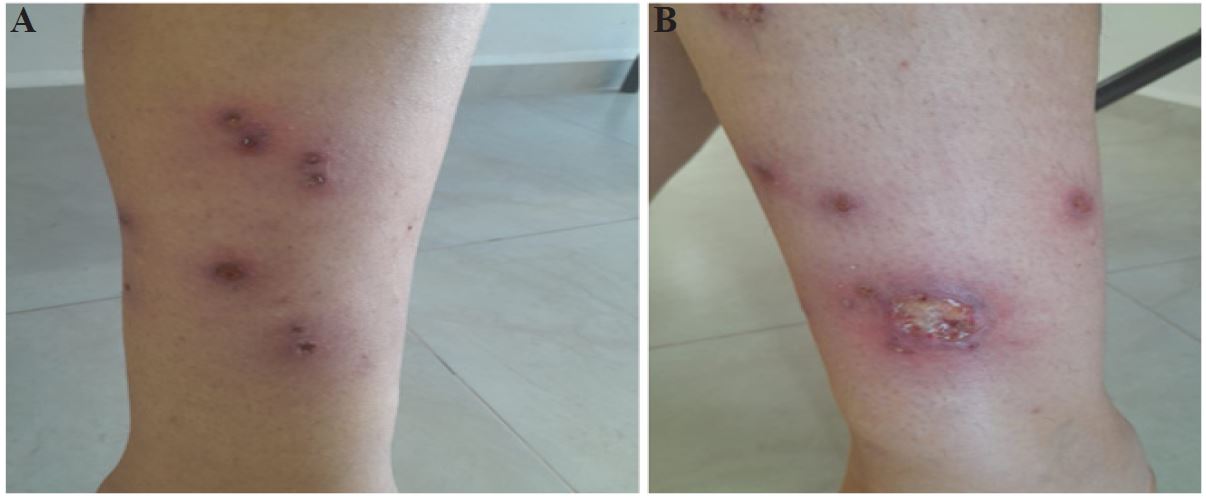

After the second loading dose (4 weeks later), the patient began to present aphthous ulcerations in the mouth and raised, maculous, reddish lesions and pustules on the arms and legs. In addition to pain in the left heel. Due to this situation and the lack of response to corticosteroid therapy, the patient was referred to hospital in March 2023.
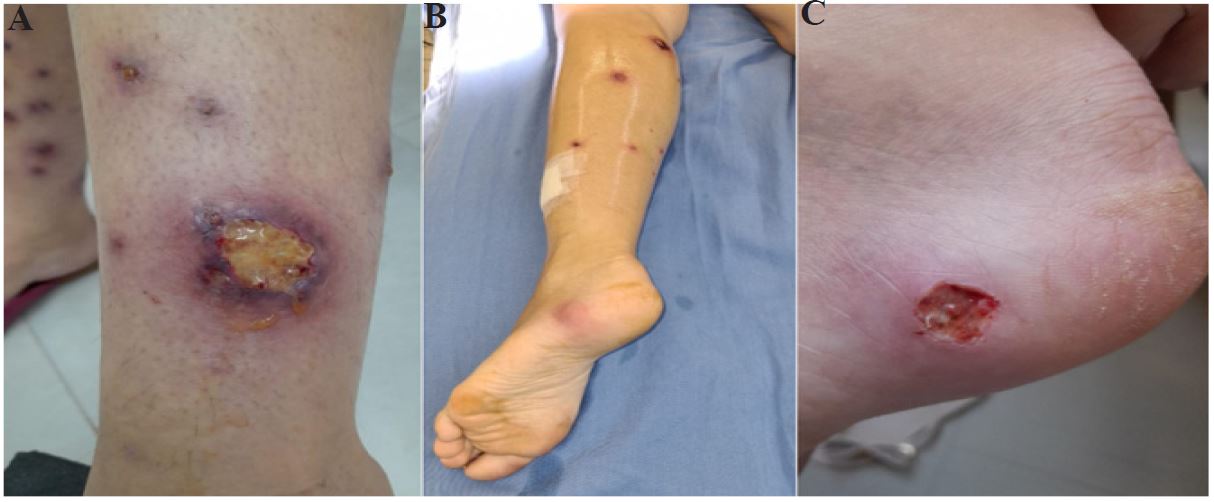
She presented severe anemia, malnutrition (loss of 13 kg in 2 months), as well as ulcerative, painful, and pustular skin lesions on the right lower limb (pyoderma gangrenosum) and erythematous lesions on the knees and arms (erythema nodosum).
In an abdominal tomography performed at the service, no significant intestinal involvement was found. The next day, an ultrasound was performed due to a suspected abscess on the left foot, which was confirmed with a collection located posterior to the lateral malleolus, on the left foot, with irregular topography, measuring 3.2x1.6x1.7 centimeters. She was taken to the surgical center for drainage of approximately 5 ml of pus, with no bacteria showing on culture (aseptic abscess). That day, the patient’s anemia worsened, and 2 packed red blood cells were infused.
During evolution, another collection appeared close to the right elbow and its evolution was observed without surgical drainage. We chose to introduce a second drug. TOFA was chosen 2 cp PO every 12 hours (loading dose), and the VDZ was maintained. After treatment, the patient’s condition improved significantly, being discharged 8 days later and returning for outpatient follow-up.
Two weeks later, the patient returns to the AMU coloproctology service for follow-up. It began with gradual withdrawal of mesalazine. There was a substantial reduction in anemia, and he still reported arthralgia in the wrists, metacarpals, knee, especially on the left, with morning stiffness. We referred the patient to the rheumatologist and the wound clinic where she was advised on the use of topical tacrolimus for pustular lesions.
Upon return, the patient, still using TOFA and VDZ, reported having been diagnosed with spondyloarthritis by the rheumatologist, but with good remission of the painful condition. At the last follow-up, in February 2024, the patient was in remission of the disease, with a good quality of life, with the lesions healed and inflammatory tests (CRP and fecal Calprotectin) normal.
Discussion
Patients with UC manifest intestinal and not infrequently extraintestinal signs and symptoms. Some of these extraintestinal manifestations occur together with intestinal symptoms while others occur independently of them.
Theoretically, drug treatments can benefit EIM based on two mechanisms of action: (1) improvement of intestinal inflammation and secondary reduction of disease-related EIM or (2) direct effects on tissue-specific mechanisms [24].
It is conceivable that VDZ has no effect on EIM because of its intestinal selective mechanism of action [25]. An overexpression of TNF-α, but not MAdCAM-1, was found in skin biopsies, suggesting that VDZ may be effective only in cutaneous EIM, thus reflecting luminal disease activity.
No controlled trials have specifically studied the efficacy of VDZ for EIM in patients with IBD, but data are available from post hoc analyzes of RCTs, prospective and retrospective cohort studies, case series, and case reports. Although musculoskeletal and hepatobiliary EIMs have been studied most extensively, data are relatively scarce. Other than erythema nodosum, there is little evidence of the effectiveness of VDZ in the treatment of skin EIM. The potential to trigger paradoxical cutaneous manifestations remains poorly characterized [26].
In a French study, paradoxical skin manifestations (i.e. psoriasis, psoriasiform eczema and eczema) were described in 4.8% of patients (14/294), half of whom (8/14) also developed paradoxical manifestations during treatment previous with TNF antagonists [25]. 27 However, it is notable that no signs for psoriasiform lesions were observed in the VDZ clinical trial program. This reported patient draws attention because she always develops an inflammatory condition during periods of relapse. Four different EIMs (pyoderma gangrenosum, erythema nodosum, aseptic abscess and spondyloarthritis) appeared concomitantly with relapse of the intestinal disease [25]. Another fact that draws attention is that the patient has failed two biological treatments and is in the induction period of a third with selective action. Cases like these illustrate well the nuances of a complicated disease and the difficulties that the doctor faces in choosing the best therapy.
Teixeira et al. em 2018, reported the case of a patient with UC treated with TOFA and previously failed three biologics with two different mechanisms of action (2 anti-TNF and VDZ) with excellent results. In 2021, with its approval in Brazil’s public health system, TOFA became a viable option for use in patients with UC, with a systemic mechanism [28].
Given this, the choice of TOFA as a second drug seems the most logical in a patient who lost response to an anti-TNF and who was still undergoing induction (second dose) of VDZ. Even more so with such an exacerbated condition and great systemic (nutritional) compromise, the use of a drug with a rapid onset of action is very appropriate.
The result was impressive with patients demonstrating clinical improvement from the first week of using the medication, combined with the use of corticosteroids. The patient was discharged from hospital after 8 days with outpatient control and after 6 weeks of treatment she was asymptomatic and with few skin lesions in the final stage of healing.
Retrospectively reviewing these data, we noticed the delay between the correct diagnosis and the start of biological therapy. A total of 3 years was lost from the onset of symptoms to the introduction of the first drug. According to a recent study by ABCD (Brazilian Association of Ulcerative Colitis and Crohn’s Disease), up to 20% of patients with IBD in Brazil take more than 3 years to be diagnosed. This is due to difficulties in accessing specialists and diagnostic tests [29]. This case was further complicated by the instability of the inflammatory condition with periods of clinical remission that suggested good control with conventional treatment, but whenever the corticosteroids were discontinued, the symptoms returned. This corticosteroid dependence is what motivated the final decision to use anti-TNF as the first option [30]. Another important aspect to report was the recurrence of the disease occurring shortly after changing the medication the patient had been using to a biosimilar medication (infliximab) or even generic medication (mesalazine). Although the symptoms return weeks after these changes, we know that there is often a loss of response with the use of medication and these events could have occurred by chance in a patient who would lose response even with the maintenance of the medication he was using, but we must warn that the quality of products varies greatly from company to company and the multiple exchanges of biosimilars still require more studies to prove their effectiveness and safety.
With this case, we want to demonstrate the difficulty of treating these patients with UC associated with several EIM. In addition to knowledge of the therapeutic arsenal, the doctor must have a multidisciplinary team to better manage these complications. This multidisciplinary approach plays an important role in the case of involvement in addition to the coloproctologist, a rheumatologist, nutritionist, and dedicated nurse.
Declarations
Collaborators: ABQ, designed the study. ABQ and VAN collected data. ABQ and VAN analyzed the data, revised and wrote the paper. All authors approved the final version.
Conflicts of interests: Quaresma AB and Neto VA have no conflicts of interest.
Funding: None.
References
- Hedin CRH, Vavricka SR, Stagg AJ, Schoepfer A, Raine T, Puig L, et al. The Pathogenesis of Extraintestinal Manifestations: Implications for IBD Research, Diagnosis, and Therapy. Journal of Crohn’s and Colitis. 2019; 13(5): 551-554.
- Ahmed MH, Elashery M, Maksoud HA, Mahros AM. Ocular Affection as an Extraintestinal Manifestation in Cases of Inflammatory Bowel Disease at the Kafrelsheikh Governorate. Journal of Coloproctology. 2021; 41(1): 008- 013.
- Antonelli E, Bassotti G, Tramontana M, Hansel K, Stingeni L, Ardizzone S, et al. Dermatological Manifestations in Inflammatory Bowel Diseases. Journal of Clinical Medicine. 2021; 10(2): 364.
- Bernstein CN, Benchimol EI, Biton A, Murthy SK, Nguyen GC, Lee K, et al. The Impact of Inflammatory Bowel Disease in Canada 2018: Extra-intestinal Diseases in IBD. Journal of the Canadian Association of Gastroenterology. 2019; 2(1): S73 -S80.
- Bouhuyus M, Armbrust W, Rheenen PF van. Case Report: Systemic Small-Vessel Vasculitis in an Adolescent with Active Ulcerative Colitis. Frontiers in Pediatrics. 2021; 9(617312).
- Buck M, Dumic I, Mcdermott W, Nordstrom C, Dawan S, Virata A, et al. Leukocytoclastic vasculitis as a rare dermatologic manifestation of Crohn’s disease mimicking cellulitis: a case report. BMC Gastroenterology. 2020; 20(240).
- Diaconescu S, Strat S, Balan GC, Anton C, Stefanescu G, Loniuc I, et al. Dermatological Manifestations in Pediatric Inflammatory Bowel. Disease. Medicina. 2020; 56(9): 425.
- Fine S. Extraintestinal Manifestations of Inflammatory Bowel Disease. Rhode Island Medical Journal. 2022; 105(9): 13-19.
- Harbord M, Annese V, Vavricka SR, Allez M, Acosta MBD, Boberg KM, et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. Journal of Crohn’s and Colitis. 2016; 10(3): 239-254.
- Hedin CRH, Sonkoly E, Eberhardson M, Stahle M. Inflammatory bowel disease and psoriasis: modernizing the multidisciplinary approach. Journal of Internal Medicine. 2021; 290(2): 25 -278.
- Kumar S, Pollok R, Goldsmith D. Renal and Urological Disorders Associated with Inflammatory Bowel Disease. Inflammatory Bowel Diseases. 2022.
- Sange AH, Sinivas N, Sarnaik MK, Modi S, Pisipati Y, Vaidya S, et al. Extra-Intestinal Manifestations of Inflammatory Bowel Disease. Cureus. 2021; 13(8): 17187.
- Shah J, Shah A, Hassman L, Gutierrez A. Ocular Manifestations of Inflammatory Bowel Disease. Inflammatory Bowel Diseases. 2021; 27(11).
- Sleiman J, Hitawala AA, Cohen B, Falloon K, Simonson M, Click B, et al. Systematic Review: Sweet Syndrome Associated with Inflammatory Bowel Disease. Journal of Crohn’s and Colitis. 2021; 15(11): 1864- 1876.
- Lee HS, Park SK, Park DI. Novel treatments for inflammatory bowel disease. The Korean Journal of Internal Medicine. 2018; 33(1): 20-27.
- Na SY, Moon W. Perspectives on Current and Novel Treatments for Inflammatory Bowel Disease. Gut and Liver. 2019; 13(6): 604-616.
- Santos CHM, Galindo ACA, Silva BA, Dantas CR, Guilherme IAA, Gomes JEBN, et al. Comparative analysis of anxiety and depression prevalence between individuals with and without inflammatory bowel disease. Journal of Coloproctology. 2020; 40(4): 339-344.
- Thomas PWA, Broeder ND, Derikx M, Kievit W, West RL, Russel MGVM, et al. Impact of Biological Therapies and Tofacitinib on Real-world Work Impairment in Inflammatory Bowel Disease Patients: A Prospective Study. Inflammatory Bowel Diseases. 2022; 28(12): 1813-1820.
- Guillo L, Abreu M, Panaccione R, Sandborn WJ, Azevedo VF, Gensler L, et al. Endpoints for extraintestinal manifestations in inflammatory bowel disease trials: the EXTRA consensus from the International Organization for the Study of Inflammatory Bowel Diseases.The Lancet. 2022; 7(3): 254-261.
- Quaresma AB, Damiao AOMC, Coy CSR, Magro DO, Hino AAF, Valverde DA, et al. Temporal trends in the epidemiology of inflammatory bowel diseases in the public healthcare system in Brazil: A large population-based study. The Lancet Regional Health – Americas. 2022; 16.
- Quaresma AB, Coy CRS, Damiao AOMC, Kaplan GG, Kotze PG. Biological therapy penetration for inflammatory bowel disease in Latin America: current status and future challenges. Arquivos de Gastroenterologia. 2019; 56(13).
- Queiroz NSF, Martins CDM, Quaresma AB, Sendra PAO, Suarez KE, Kotze PG. IBD barriers across the continents: a continent-specific analysis: Latin America. Therapeutic Advances in Gastroenterology. 2023; 16.
- Vilela EG, Rocha HC, Moraes AC, Santana GO, Parente JM, Sassaki LY, et al. Inflammatory bowel disease care in Brazil: how it is performed, obstacles and demands from the physicians’ perspective. Arquivos de Gastroenterologia. 2020; 57(4).
- Lakatos L, Pandur T, David G, Balogh Z, Kuronya P, Tollas A, et al. Association of extraintestinal manifestations od Inflammatory Bowel Disease in a province of western Hungary with disease phenotype: results of a 25-year follow-up study. Word J Gastroenterol. 2003; 2300-7.
- Hanzel J, Ma C, Casteele NV, Khanna R, Jairath V, Feagan BG. Vedolizumab and Extraintestinal Manifestations in Inflammatory Bowel Disease. Drugs. 2021; 81(3): 333-347.
- Lissner D, Glauben R, Allers K, Sonnenberg E, Loddenkemper C, Schneider T, et al. Pulmonary manifestation of Crohn’s disease developed under treatment with vedolizumab. Am J Gastroenterol. 2018; 113(1): 146-148.
- Tadbiri S, Peyrin-Biroulet L, Serrero M, Filippi J, Pariente B, Roblin X, et al. Impact of vedolizumab therapy on extra-intestinal manifestations in patients with infammatory bowel disease: a multicentre cohort study nested in the OBSERV-IBD cohort. Aliment Pharmacol Ther. 2018; 47(4): 485-493.
- Teixeira FV, Damião AOMC and Kotze PG. Tofacitinib in the management of ulcerative colitis refractory to anti-TNF and anti-integrin therapies Arq. Gastroenterol. 2018; 55(2).
- Machado MB, Vieira A, Steinwurz F, Vasconcelos MIL, Zaltman C, Quintiliano P, et al. Jornada do paciente com Doença Inflamatória Intestinal. Estudo quantitativo e qualitativo sobre a vida do paciente com DII no Brasil. www.abcd.org.br. No prelo. 2017.
- Balderramo D, Quaresma AB, Olivera PA, Savio MC, Villamil MPG, Panaccione R, Ng SC, Kaplan GG, Kotze PG. Challenges in the diagnosis and treatment of inflammatory bowel disease in Latin America. Lancet Gastroenterol Hepatol. 2024; 9(3): 263-272.