
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Unusual presentation of sarcomatoid mesothelioma in a young female
Prashanth Reddy Yella1*; Simhachalam Gurugubelli2; Ravi Jagani3; Nihar Jena4
1Department of Internal Medicine, Yuma Regional Medical Center, Yuma, Arizona, USA.
2Department of Internal Medicine, Memorial Physicians Clinic, St. Louis, Mississippi, USA.
3Department of Family Medicine, Yuma Regional Medical Center, Yuma, Arizona, USA.
4Department of Cardiology, St Joseph Mercy Oakland, Michigan, USA.
*Corresponding Author : Prashanth Reddy Yella
Department of Internal Medicine, Yuma Regional Medical Center, Yuma, Arizona, USA.
Email: prashanthreddy2179@gmail.com
Received : Apr 18, 2024
Accepted : May 13, 2024
Published : May 20, 2024
Archived : www.jcimcr.org
Copyright : © Yella PR (2024).
Citation: Yella PR, Gurugubelli S, Jagani R, Jena N. Unusual presentation of sarcomatoid mesothelioma in a young female. J Clin Images Med Case Rep. 2024; 5(5): 3060
Description
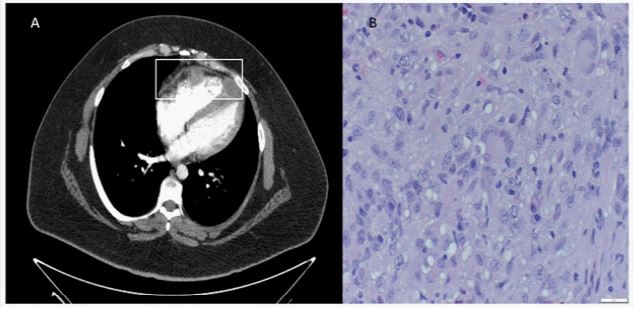
A 24-year-old female with a history of smoking presented with substernal chest pain radiating to her left arm. She also reported dysphonia for 2 weeks. She denied any shortness of breath, sore throat, cough, or fever. On physical examination, she had normal lung and heart sounds. Labs were unremarkable. Computed tomogram of the chest showed evidence of multiple enlarged hilar and mediastinal lymph nodes with multiple intracardiac lesions adherent to the myocardial wall (Figure 1A). An echocardiogram with contrast showed 2 or 3 nodular echo-densities in the right ventricular myocardium, findings that were suspicious for cardiac sarcoidosis. Cardiothoracic surgery was consulted, and the patient underwent flexible bronchoscopy, right minimally invasive thoracotomy, and mediastinal mass biopsy. The final histopathology report confirmed sarcomatoid mesothelioma (Figure 1B). On further questioning, patient denied any asbestos exposure. The patient was started on dual checkpoint immunotherapy by the oncologist. Restaging CT scan at 6-month follow-up showed interval worsening of the disease, but still within the definition of stable disease. She has been following up closely with the oncologist as an outpatient. Sarcomatoid mesothelioma is a fatal malignancy originating from the lining cells (mesothelium) of the pleural and peritoneal cavities [1]. More than 80% of all mesotheliomas originate in the pleura and are frequently associated with a history of asbestos exposure [2]. Mesothelioma is primarily a disease of adults and usually presents in the fifth to seventh decades, with 70–80% of cases occurring in men [1]. Majority of pleural mesotheliomas (90%) present with symptoms of shortness of breath and chest pain [3]. Rarer manifestations include phrenic nerve palsy, irritative cough, hoarseness of voice, and spontaneous pneumothorax [3]. Tumors metastatic to the heart are among the least known in oncology [4]. In this case, we present a young woman with a rare presentation of sarcomatoid mesothelioma with metastasis to the myocardium and without any asbestos exposure.
References
- Moore AJ, RJ Parker, J Wiggins. Malignant mesothelioma. Orphanet J Rare Dis. 2008; 3: 34.
- Neumann, V., et al., Malignant pleural mesothelioma: incidence, etiology, diagnosis, treatment, and occupational health. Dtsch Arztebl Int. 2013; 110(18): 319-26.
- Bianco, A., et al., Clinical diagnosis of malignant pleural mesothelioma. J Thorac Dis. 2018; 10(Suppl 2): S253-s261.
- Bussani R, et al. Cardiac metastases. J Clin Pathol. 2007; 60(1): 27-34.