
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Actinomycosis: A benign infection with aggressive behavior about 16 cases
Maadane Amina1*; Slimani F1,6; Satlane S2; Adnane F2,6; Ailalm F2,6; Ouggane I3; Ihbibane F3,6; Marhoum El Filali K3,6; Salam S4,6; Chlyah A5,6; Jouhadi Z2,6
1Department of Stomatology and Maxillofacial Surgery, Ibn Rochd University Hospital Center, BP, 2698, Casablanca, Morocco.
2Department of Pediatric Infectious Diseases, Ibn Rochd University Hospital Center, Casablanca, Morocco.
3Department of Infectious Diseases, Ibn Rochd University Hospital, Casablanca, Morocco.
4Pediatric Radiology Department, Ibn Rochd University Hospital, Casablanca, Morocco.
5Pediatric Dentistry Department, Ibn Rochd University Hospital, Casablanca, Morocco.
6Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, BP, 5696, Casablanca, Morocco.
*Corresponding Author : Amina Maadane
Department of Stomatology and Maxillofacial Surgery, CHU Ibn Rochd, BP, 2698, Casablanca, Morocco.
Tel: +212 696321597;
Email: Aminamaadane8@gmail.com
Received : Apr 29, 2024
Accepted : May 16, 2024
Published : May 23, 2024
Archived : www.jcimcr.org
Copyright : © Maadane A (2024).
Abstract
Introduction: Actinomycosis is a rare bacterial infection, characterized by chronic and progressive granulomatous inflammation, caused by Gram-positive anaerobic bacilli: Actinomyces. The most frequently incriminated species is Actinomycete israeli. The diagnosis of actinomycosis is essentially anatomo-pathological and the cervico-facial location is the most common. The objective of our study is to report the epidemiological, clinical, radiological, therapeutic and evolving profile of actinomycosis through a series of 16 cases and to draw the attention of practitioners to this often little-known pathology whose diagnosis is often done histologically by Chance when taking a sample during a surgical procedure.
Materials and methods: Our study is retrospective, descriptive including 16 patients in whom the diagnosis of actinomycosis was confirmed, all locations combined, over a period from September 2019 to April 2022.
Results: The average age of patients was 36 years, with a slight female predominance (7M/9F). The location was cervico-facial in 12/16 cases, thoraco-pulmonary in 2 cases, abdominopelvic, and femoral bone each in one case.
The portal of entry was mainly oral. The clinical symptoms were dominated by chronic suppuration in 14 cases, and a pseudo-tumor appearance in 11. The most frequently encountered radiological signs were an infiltrated appearance of the soft tissues with or without abscessed collection. The diagnosis was confirmed by anatomo-pathological analysis of the surgical specimens in all our patients.
All our patients received treatment with penicillin G or penicillin A with an average treatment duration of 4 months (1 month - 2 years). Nine patients required surgical intervention. Complete recovery was noted in 12 patients.
Conclusion: The diagnosis of actinomycosis remains difficult and often unknown to practitioners, due to its polymorphous clinical and radiological presentations leading to confusion with other pathologies, particularly infectious or tumoral. Its management is based on antibiotic therapy at high doses and of prolonged duration, often associated with surgical action.
Keywords: Actinomyces; Actinomycosis; Diagnosis; Treatment.
Citation: Maadane A, Slimani F, Satlane S, Adnane F, Ailalm F, et al. Actinomycosis: A benign infection with aggressive behavior about 16 cases. J Clin Images Med Case Rep. 2024; 5(5): 3070.
Introduction
Actinomycosis is a rare chronic granulomatous infection caused by filamentous Gram-positive bacilli: Actinomyces. The infection was first reported in 1877 by pathologist Otto Bollinger. It is characterized by chronic suppurative inflammation with the formation of fistulas and a discharge of yellowish pus. There are more than 30 species of Actinomyces identified, the majority of infections are caused by Actinomyces israelii and Actinomyces genencseriae [1,2]. These bacteria mainly belong to the human commensal flora of the oropharynx, gastrointestinal tract and urogenital tract. Some become pathological when the mucosal barrier is broken. The most common locations of actinomycosis are: orocervical (60%), abdominal (20%), pulmonary (15%) and pelvic (5%). The least common sites of actinomycotic infection are the central nervous system, musculoskeletal tissues. Very cases of disseminated forms have been reported [2].
Depending on the anatomical site affected, actinomycosis can manifest with various symptoms, including local pain, swelling, fever and systemic manifestations; it often mimics tumor pathology [3], tuberculosis or nocardiosis due to its chronicity, its extensive invasive nature often with the formation of cold abscesses [4]. In this work, we describe the epidemiological, clinical, radiological, therapeutic and evolutionary profile of actinomycosis through the data of our series of 16 cases including three illustrated observations.
Methods
This is a retrospective descriptive study carried out within the maxillofacial surgery department and in the adult and pediatric infectious diseases departments of the Ibn Rochd University Hospital in Casablanca. We included in our study all patients with confirmed actinomycosis treated at the aforementioned services, from September 2019 to April 2022. Epidemiological, clinical, paraclinical, therapeutic and evolutionary data were collected from patients’ medical files. These data were entered and analyzed using the software: Excel 2016.
Results
We collected 16 cases of confirmed actinomycosis. The average age of the patients was 36 years with a range of 9 to 72 years. There were 9 female patients and 7 patients (7M/9F). The mandibular location was predominant noted in 11/16 cases, then maxillary , pulmonary, thoracic, abdominal and femoral bone each in 1 case (Table 1).
The portal of entry was oral in 12 cases. The contributing factors were: oral trauma in 11 cases, alcohol and smoking in 5 patients, and immunosuppression in 3 cases (Table 2). The clinical symptoms were dominated by suppuration in 14/16 cases, painful swelling in 11 cases, a febrile context in 10 patients and a deterioration in general condition in 3 cases. The progression towards tissue necrosis was noted in 3 patients, the extension of the swelling towards the tonsillar compartment causing dysphagia in only one patient. Maxillary intra-sinus extension was noted in only one case. Chest pain, dyspnea and cough were the main symptoms noted in the 2 cases with pulmonary involvement. The abdominal location was revealed by a pseudo-surgical syndrome. The most frequently encountered radiological signs were an infiltrated appearance of the soft tissues with or without abscessed collection in 11 patients and bone lesions of osteolysis and bone sequestration in 7 patients. The biological data were little disturbed apart from bacterial superinfection. In fact, the average value of C-reactive protein and leukocytes at the time of diagnosis were respectively 59.2 mg/dl (16 to 390), and 7720/mm3 (2250 to 13000). Epidemiological, clinical and biological data are summarized in Table 1. The final diagnosis was established by pathological examination in all our patients, based on the histological identification of actinomycotic sulfur granules, with gram-positive bacilli radiating from these granules. All our patients had received treatment based on penicillin G or penicillin A with an average treatment duration of 4 months (1 month - 2 years) of which 9 had required surgery which consisted of drainage of pus, necrosectomy and excision of fistulas. The evolution was marked by complete recovery in 12/16 patients, recurrence in 3 patients and a single case of death at home.
We present below as illustrations 3 clinical observations of actinomycosis: maxillary (case no. 1), pulmonary (case no. 2) and parascapular (case no. 3).
Case no. 1
Young girl aged 14 with no particular history who presented with a right palatal ulcero-necrotic lesion noted following the extraction of tooth 16 by an unqualified technician (Figure 1). Maxillofacial CT scan (CT) revealed necrosis of the alveolar bone with infiltration of the adjacent cheek soft tissues (Figure 2).
The initial treatment consisted of the extraction of the teeth next to the lesion, the elimination of the necrotic bone which was sent for a histopathological examination which confirmed the diagnosis of actinomycosis. The patient was started on amoxicillin and metronidazole parenterally (IV) then switched to oral amoxicillin. The evolution was marked by the reappearance of ulcerative lesions after 4 months of treatment with a greater extension to adjacent soft tissues and even to the maxillary sinuses. The antibiotic treatment was undertaken with penicillin G at a rate of 200,000 IU/kg/day intravenously for 3 weeks then the relay was carried out with oral penicillin V with coinciding intervals of IV penicillin G courses. with school holidays so as not to hinder his education. The evolution was very favorable under this protocol after 6 months (Figure 3). Note that the treatment of this child was multidisciplinary, involving the maxillofacial surgeon, the dental surgeon and the pediatric infectious disease specialist.



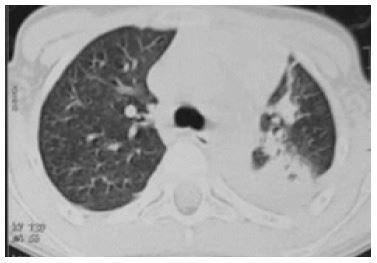
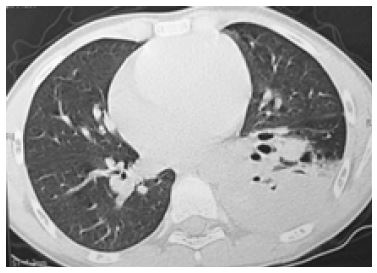
Case no. 2
A 10 year old boy, consulted for recurrent episodes of pneumonia with a fever, left chest pain, productive cough with purulent sputum; more abundant during exercise, associated with bouts of dyspnea. A fever of 40°, the respiratory examination revealed rumbling rales on the left; very poor dental condition. Chest x-ray (Rx) (Figure 1) showed a left white lung appearance.Chest CT showed condensation of the entire left lung with the presence of a right pulmonary nodule (Figure 2). An initial rigid bronchoscopy showed a whitish material obstructing the lumen of the left main bronchus and its divisions that fragments when manipulated. Several samples were sent for microbiological examination (usual pathological germs, tuberculosis bacilli and especially fungal infectious agents. Two weeks later, another bronchoscopy was undertaken due to an attack of suffocation. It revealed a recurrence of the obstruction of the lumen of the left main bronchus previously completely cleaned with extension of the whitish material to the lumen of the right main bronchus via the tracheal carina. The child again undergoes intensive cleaning with extraction of a maximum of whitish membranes. The child received parenteral antibiotic therapy for 28 days (amox-acidclav) and was discharged with a normal respiratory condition and a substantially normal chest x-ray (Figure 3). The various samples taken endoscopically were all negative. aspergillus, hydatid and candida serologies were also all negative. And a field assessment looking for primary or secondary immunodeficiency was negative. The child did not consult again until a year later when he experienced a new episode of respiratory difficulty. The CT scan: showed a focus of alveolar condensation in the left upper lobe (Figure 4). Resumption of a third bronchoscopy with bronchoalveolar washing; many samples were again referred for bacteriological and mycological examination. Mycological examination revealed Actinomyces sp. With two other germs: a Bifidobacterium Sp and a lactobacillus acidophilus!! The child was then placed on protected amoxicillin and azithromycin for 6 weeks and was released on long-term amoxicillin. The child was lost to follow-up again and returned 1 year later, a 4th bronchoscopy was performed; he objectified the presence at the level of the left bronchi of two large plugs of pus, very solidified: the first obstructs the segmental bronchus of the Nelson segment and the second the lateral segmental bronchus of the basal pyramid. These plugs, made up of clumps of pus, were removed with forceps and suctioned several times, but these two bronchi could not be completely cleared. All samples taken during this endoscopy; they have all been negative. In January 2020; the child reports morning bronchorrhea with chronic cough. Chest radiography showed a dense and homogeneous but poorly defined opacity of the left upper lobe (Figure 5). On chest CT, we noted the presence of multiple dense nodules of the left upper lobe of variable size and total condensation of the left lower lobe with a focus of bronchiectasis (Figure 6). A final control bronchoscopy did not reveal any whitish membranes but just purulent secretions linked to the infected bronchiectasis site; the samples taken were negative. This patient proposed for a cure of his bronchiectasis.
Case no. 3
Little girl aged 9, without any particular pathological history. The history of his illness dates back 6 months before his hospitalization with pain in the posterior aspect of the right shoulder with the progressive appearance of a dorsal swelling over 1 month. The clinical examination revealed aright parascapular mass, painless, firm fixed in relation to the deep plane, poorly limited, measuring 14.3 cm, without inflammatory signs adjacent to it or fistulization to the skin with the presence of 2 other adjacent painless masses of the same mobile appearance, subcutaneously measuring 1.1 cm. This symptomatology evolved in a context of apyrexia and deterioration of general condition without other associated physical abnormalities. An MRI as well as a TAP CT were carried out and have revealede a right posterolateral chest wall tissue mass with underlying rib lysis and presence of right pulmonary nodules without secondary lesions at the abdominal levele (Figure 1). The diagnosis of Ewing sarcomawas raised, however, a surgical biopsy of the bone and soft tissues showed an inflammatory reactionhistiocytic and neutrophilic around actinomycosis grains without tumor proliferation. The evolution was marked by the regression of the tumor mass under long-term antibiotic therapy alone based on penicillin G (Figure 2).
Table 1: Clinical and biological epidemiological data from our series.
| Case | Age | Sex | Location | Clinical signs | Biology |
|---|---|---|---|---|---|
| n1 | 60 | F | Mandible | Fistulized gingival swelling with pus | CRP=45 GB=9000 |
| n2 | 37 | F | Mandible | Fever, painful swelling | CRP=56 GB=6200 |
| n3 | 69 | F | Mandible | Fever, alteration of general condition(AGC),purulent gingival lesion, jugal edema; | CRP=20 GB=6200 |
| n4 | 14 | F | Mandible | Purulent ulcerative mucosal lesion | CRP=36 GB=6200 |
| n5 | 16 | F | Mandible | Fever, fistulized gingival swelling with pus | CRP=26 GB=7200 |
| n6 | 25 | F | Mandible | Swelling on indurated mucosal lesion with pusdischarge | CRP=86 GB=5300 |
| n7 | 19 | M | Mandible | Fever fistulized mucosal lesion trismus | CRP=59.2 GB=5190 |
| n8 | 63 | M | Mandible | Purulent ulcerative mucosal lesion | CRP=100 GB=13000 |
| n9 | 50 | M | Mandible | Fever, AGC, ulcerated lesion bone exposure necrosis,trismus | CRP=100 GB=8360 |
| n10 | 58 | M | Mandible | Fever Ulcero-purulent mucosal lesion | CRP=60 GB=7500 |
| n11 | 72 | M | Mandible | Jugal swelling, skin fistula, purulent gingivalulceration | CRP=16 GB=2500 |
| n12 | 41 | M | Abdomen | Fever, abdominal pain, hepatosplenomegaly andascites | CRP=215 GB=2250 |
| n13 | 22 | F | Femur | Inflammatory pain in the left hip on totalprosthesis | CRP=130 GB=13000 |
| n14 | 10 | M | Lung | Fever, chest pain, dyspnea, purulent cough | CRP=390 GB=12500 |
| n15 | 9 | F | Thoracic | Painful right parascapular mass | CRP=40 GB=11000 |
| n16 | 14 | F | Maxillary; | Ulcero-necrotic lesion of the palate, with pusdischarge; | Negative CRP GB=11150 |
| Total (n=16) | 7M/9F | 11mandibular/1maxillary/2 pulmonary/1thoracic/1abdominal/1femoral | |||
Table 2: Actinomycosis risk factors found in our patients.
| Field of occurrence | >Number |
|---|---|
| Dental procedure | 13 |
| Mucous wound | 1 |
| Osteitis | 7 |
| Diabetes | 4 |
| Immunosuppression | 3 |
| Tumors | 4 |
| Smoking | >5 |






Discussion
Actinomyces species are part of the commensal flora of the mucous membranes, oral, respiratory, digestive and genital. In the human oral cavity, Actinomyces live as endosaprophytes in gingival crevices, tonsillar crypts, periodontal pockets, in dental plaques and decayed teeth. No environmental reservoir such as soil has been documented, and it does not there is no human-to-human transmission of Actinomyces [5,6].
Actinomyces infection generally begins after breakdown of the mucosal barriers and then spreads by contiguity, but also by hematogenous rather than lymphatic dissemination, to numerous distant organs or tissues. Once Actinomyces invades tissue, it develops a chronic granulomatous infection characterized by the formation of tiny clumps, called sulfur granules because of their yellow color (2.5).
This infection is often late diagnosed because it can mimic other conditions such as malignancies and tuberculosis (4,7.8). Indeed, many cases of actinomycosis initially diagnosed as tumors or other serious illnesses are reported in the medical literature [2,9-13,15,16].
Actinomycosis has been described in all age groups and all types of patients, both immunocompetent and immunocompromised, but it seems to be more common in young adults (20-60 years and often between 30 and 50 years), advantage in men (2.8). In our series we observed 7H/9F.
The incidence of all forms of actinomycosis is thought to have declined in recent years, particularly in developed countries due to improved oral hygiene and susceptibility to a wide range of antibiotics [7].
The oro-cervico-facial location represents the most common form of the disease and constitutes 50% of all cases reported in the literature [7] observed in 12/16 cases in our series. Certain conditions predispose to the appearance of this form, notably caries and dental extractions by non-professionals, gingivitis and gingival trauma, infections of erupting teeth, chronic tonsillitis, otitis or mastoiditis, diabetes, immunosuppression, malnutrition, and local tissue damage caused by surgery, neoplastic disease, or irradiation [4,17,18]. Most of these factors were found in the history of our patients, mainly the history of dental care (in 13 cases/16).
Cervicofacial actinomycosis generally affects the tissues surrounding the maxilla or mandible, including bone tissue in approximately 50% of cases, the cheek (15%), chin (15%), ramus and submandibular region (10%). More rarely, the mandibular joint may be affected [4]. Infections of the nose, paranasal sinuses, oropharynx, hypopharynx, tongue, and trachea may also be seen [5,7,9].
Typically, the disease presents as an indurated, painless, slowly progressive mass, progressing to multiple abscesses with draining fistulas on the surface of the skin or oral mucosa, sometimes expressing a typical thick yellow exudate with characteristic sulfur granules [2,4,19], this form was predominant in our series with the presence of suppurative lesions in 14/16 cases. In advanced stages, pain and trismus can appear due to infiltration of the masticatory muscles (observed in two cases of mandibular actinomycosis in our series).
Thoracopulmonary actinomycosis represents 15 to 20% of cases with only 2/16 cases reported in our series. Infection normally results from aspiration of oropharyngeal secretions, but it can also occur after esophageal perforation, local spread from head and neck or abdominal infection, or hematogenous spread [4]. The disease is most often diagnosed in the chronic phase, as its symptoms are similar to those of other chronic lung infections such as tuberculosis or thoracic cancer: productive cough, hemoptysis, dyspnea and chest pain. General symptoms such as weight loss, fever and night sweats may be present in pulmonary localization [4,10,11,19].
The abdominopelvic localization of actinomycosis represents 20% of cases, it is generally insidious, can affect all organs and simulate pathologies such as diverticulitis, appendicitis, inflammatory bowel diseases and malignant tumors, among others it is often accompanied by nonspecific symptoms such as fever, weight loss, and abdominal pain. A mass is not always palpable [12-15,19].
Although abdominal disease can spread directly to the pelvis, pelvic actinomycosis is primarily associated with intrauterine contraceptive devices. The duration of use necessary to increase the risk of infection is not yet known [17,18].
Other rare sites of actinomycosis include the central nervous system, bone, muscle tissue, and prosthetic joints [2,4,6,7,19].
The distinction between actinomycosis and neoplastic pathology and other infections, particularly of mycobacterial, fungal or parasitic origin, constitutes real difficulties in differential diagnosis.
During non-superinfected actinomycosis, the biological inflammatory syndrome is little disturbed or even normal. Imaging methods such as conventional radiography, computed tomography and Magnetic Resonance Imaging (MRI) do not make it possible to make a precise diagnosis, but allow us to define more precisely the dimensions and extent of the infection [7,10,20].
Histological examination and bacterial culture of an abscess or bone suspected of osteomyelitis constitute the gold standard for the diagnosis of actinomycosis. Clinicians should report suspected actinomycosis to the microbiologist to ensure that prolonged culture on appropriate media and in an adequate atmosphere is performed. Also, it is recommended to perform several biopsies at different tissue levels in order to improve the histopathological diagnosis. The observation of yellowish sulfur granules which are made up of a conglomerate of bacteria trapped in a biofilm is very suggestive of actinomycosis [2,4-6].
Treatment is based on the administration of high doses of amoxicillin (up to 200 mg/kg/day) or penicillin G (up to 24 MIU/day) intravenously in severe cases. Acceptable alternatives are clindamycin, macrolides and doxycycline, the latter has better bone penetration. The addition of a complementary medication such as metronidazole or a beta-lactamase inhibitor is justified in cases of suspected bacterial superinfection by non-specific germs [2,7].
Surgical management may be necessary for drainage of large abscesses, excision of fibrotic lesions, debridement of necrotic bone tissue in cases of osteomyelitis. Treatment of dental caries and/or apical abscesses is essential and often requires dental avulsions [4,14-16]. Medical treatment, which can last up to 6 to 12 months, can be shortened if optimal surgical resection of infected tissue has been performed. However, treatment should always be continued long enough after all clinical signs have disappeared to avoid recurrence [1,2,4,5]. Our case series offers a valuable overview of the various clinical manifestations of actinomycosis, notably the intraoral involvement which has been the most reported, which is consistent with the data in the literature; this can be explained by the poor oral condition in a good part of our population. The clinical presentation often simulates a tumor origin, especially in the absence of suppurative and granulomatous character, which may be the subject of unnecessary investigations and procedures and delayed treatment.
Conclusion
It is important to consider this rare pathology in the differential diagnosis of patients presenting infectious and/or pseudo-tumor symptoms and to adopt a comprehensive evaluation strategy integrating histopathological examination alongside clinical examination and imaging. Early detection allows medical treatment and a high chance of recovery without the need for invasive procedures.
Expression of interest: All authors declare that they have no conflict of interest in this work.
References
- Boot M, Archer J, Ali I. The diagnosis and management of pulmonary actinomycosis. J Infect Public Health. 2023; 16(4): 490-500. doi: 10.1016/j.jiph.2023.02.004. Epub 2023 Feb 8. PMID: 36801629.
- Boyanova L, Kolarov R, Mateva L, Markovska R, Mitov I. Actinomycosis: a frequently forgotten disease. Future Microbiol. 2015; 10(4): 613-28. doi: 10.2217/fmb.14.130. PMID: 25865197.
- Anannamcharoen S, Nimmanon T, Boonya-Ussadorn C. Abdominal actinomycosis mimicking colon cancer. Asian J Surg. 2023; 46(3): 1536-1538. doi: 10.1016/j.asjsur.2022.09.069. Epub 2022 Oct 15. PMID: 36253265.
- Valor F, Sénéchal A, Dupieux C, Karsenty J, Lustig S, Breton P, Gleizal A, Boussel L, Laurent F, Braun E, Chidiac C, Ader F, Ferry T. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014; 7: 183-97. doi: 10.2147/IDR.S39601. PMID: 25045274; PMCID: PMC4094581.
- Oostman O, Smego RA. Cervicofacial Actinomycosis: Diagnosis and Management. Curr Infect Dis Rep. 2005; 7(3): 170-174. doi: 10.1007/s11908-005-0030-0. PMID: 15847718.
- Schaal KP, Lee HJ. Actinomycete infections in humans--a review. Embarrassed. 1992; 115(1-2): 201-11. doi: 10.1016/0378-1119(92)90560-c. PMID: 1612438.
- Wong VK, Turmezei TD, Weston VC. Actinomycosis. BMJ. 2011; 343: d6099. doi: 10.1136/bmj.d6099. PMID: 21990282.
- Skuhala T, Vukelić D, Desnica B, Balen-Topić M, Stanimirović A, Višković K. Unusual presentations of actinomycosis: a case series and literature review. J Infect Dev Ctries. 2021; 15(6): 892-896. doi: 10.3855/jidc.13414. PMID: 34242202.
- Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015; 28(2): 419-42. doi: 10.1128/CMR.00100-14. PMID: 25788515; PMCID: PMC4402957.
- Aydin Y, Arslan R, Filik M. Pulmonary actinomycosis mimicks lung cancer. Rev Soc Arm Med Trop. 2022; 55: e0195. doi: 10.1590/0037-8682-0195-2022. PMID: 35976334; PMCID: PMC9405929.
- Loukil M, Khalfallah I, Bouzaidi K, Chelbi E, Ghrairi H. Pulmonary actinomycosis. Diagnostic and therapeutic features [Pulmonary actinomycosis. Diagnostic and therapeutic features]. Rev Pneumol Clin. 2018; 74(6): 508-513. French. doi: 10.1016/j.pneumo.2018.05.001. Epub 2018 May 30. PMID: 29859741.
- Jabi R, Ramdani H, Elmir S, Elmejjati F, Serji B, El Harroudi T, Bouziane M. Pseudotumoral Actinomycosis Mimicking Malignant Colic Disease: A Case Report and Literature Review. Visc Med. 2020; 36(4): 333-337. doi: 10.1159/000502895. Epub 2019 Oct 14. PMID: 33005660; PMCID: PMC7506202.
- Belhamdiya, Meriam, Rajae Afifi, Imane Benelbarhdadi, FZ Ajana and Abdellah Essaid. “Abdominopelvic actinomycosis: diagnostic and therapeutic difficulties.” Acta Endoscopica 34 (2004): 431-436.
- Lisa-Gracia M, Martín-Rivas B, Pajarón-Guerrero M, Arnáiz-García A. Abdominal actinomycosis in the last 10 years and risk factors for appendiceal actinomycosis: review of the literature. Turk J Med Sci. 2017; 47(1): 98-102. doi: 10.3906/sag-1511-52. PMID: 28263474.
- McFarlane ME, Coard KC. Actinomycosis of the colon with invasion of the abdominal wall: An uncommon presentation of a colonic tumor. Int J Surg Case Rep. 2010; 1(1): 9-11. doi: 10.1016/j.ijscr.2010.07.002. Epub 2010 Aug 26. PMID: 22096664; PMCID: PMC3199683
- de Andrade AL, Novaes MM, Germano AR, Luz KG, de Almeida Freitas R, Galvão HC. Acute primary actinomycosis involving the hard palate of a diabetic patient. J Oral Maxillofac Surg. 2014; 72(3): 537-41. doi: 10.1016/j.joms.2013.08.006. PMID: 24528563.
- Choi MM, Baek JH, Lee JN, Park S, Lee WS. Clinical features of abdominopelvic actinomycosis: report of twenty cases and literature review. Yonsei Med J. 2009; 50(4): 555-9. doi: 10.3349/ymj.2009.50.4.555. Epub 2009 Aug 19. Erratum in: Yonsei Med J. 2009 Oct 31; 50(5): 737. Beak, Jeong Heum [corrected to Baek, Jeong Heum]. PMID: 19718405; PMCID: PMC2730619.
- Chelli D, Hassini A, Aloui F, Sfar E, Zouaoui B, Chelli H, Chanoufi B. Pelvic actinomycosis Tunisian experience: about 5 cases [Pelvic actinomycosis in Tunisia: five cases]. Health. 2008; 18(2): 77-82. French. doi: 10.1684/san.2008.0107. PMID: 19188130.
- Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015; 28(2): 419-42. doi: 10.1128/CMR.00100-14. PMID: 25788515; PMCID: PMC4402957.
- Skuhala T, Vukelić D, Desnica B, Balen-Topić M, Stanimirović A, Višković K. Unusual presentations of actinomycosis: a case series and literature review. J Infect Dev Ctries. 2021; 15(6): 892-896. doi: 10.3855/jidc.13414. PMID: 34242202.