
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
The effects of photobiomodulation therapy plus methacrylate powder dressing (Altrazeal powder) on the bacterial count in diabetic foot ulcer: A case report
Lena Elahe Motamedi Nasab1; Ladan Arab Yaqoubi2; Houssein Ahmadi3*
1Department of Pediatrics, Mofid Children Hospital, Shahid Beheshti University of Medical Sciences (SBMU), Tehran, Iran.
2Rehabilitations Sciences Research Center, Zahedan University of Medical Sciences, Zahedan, Iran.
3Department of Biology and Anatomical Sciences, Shahid Beheshti University of Medical Sciences (SBMU), Tehran, Iran.
*Corresponding Author : Houssein Ahmadi
Department of Biology and Anatomical Sciences, Shahid Beheshti University of Medical Sciences (SBMU), Tehran, Iran.
Tel: +98-21-2244339 Z & +98-9123023719;
Email: Hosseinahmadi9213@yahoo.com
Received : May 01, 2024
Accepted : May 20, 2024
Published : May 27, 2024
Archived : www.jcimcr.org
Copyright : © Ahmadi H (2024).
Abstract
Diabetes patients frequently experience a serious complication known as impaired wound healing, which increases the likelihood of foot infection and limb amputation. Investigators have been looking for novel methods to treat Diabetic Foot Ulcers (DFU) recently. In this case present case, we used Altrazeal powder and photobiomodulation therapy to treat and speed up the healing of a harsh diabetic foot ulcer in a 55-year-old man with type 1 diabetes and heart failure.
We observed that the ulcer area significantly decreased as combination therapy progressed, and Within 20 weeks, the wound was healed. The pain and microbial flora were also reduced. This revealed contextual analysis demonstrated the useful effect of the mix of photobiomodulation treatment and Altrazeal powder for recuperating a serious DFU in a diabetic patient with type 1. To confirm the findings, additional clinical trials in a clinical setting are recommended. In addition, it is recommended that additional research using preclinical models uncover the combination therapy’s mechanism of action.
Keywords: Photobiomodulation therapy; Wet wound dressing; Diabetic foot infection; Wound remedy; Sareus.
Citation: Nasab EM, Yaqoubi LA, Ahmadi H. The effects of photobiomodulation therapy plus methacrylate powder dressing (Altrazeal Powder) on the bacterial count in diabetic foot ulcer: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3075.
Introduction
A metabolic disorder called Diabetes Mellitus (DM). which lasts a long time and is hard on the body. It affects people, their families, and society as a whole [1]. There are approximately 463 million people worldwide who have DM and this number is expected to rise by 25% by 2030 [2].
The body’s metabolic activity is disrupted, resulting in a delay in wound healing, and this disease raises the risk of infection. DM patients account for nearly 60% of all amputations of the whole limb [3,4]. Leg amputations are almost always preceded by an infected Diabetic Foot Ulcer (DFU) [5]. Infected DFUs are primarily associated with Staphylococcus aureus [6]. Misuse of antibiotics, particularly in patients with DFUs, has been linked to an increase in drug-resistant microorganisms [7]. Diabetic Neuropathic Pain (DNP) is a frequent issue of both type 1 and type 2 diabetes, affecting more than 90% of diabetics [8]. Poorly managed hyperglycemia can lead to peripheral neuropathy, hypoxia, inflammation, and ischemia, which can cause foot deformities and DFU. DFUs are regarded as a major health issue [9].
During diabetic wound healing, Photobiomodulation Therapy (PBMT) reduces inflammation, stimulates wound healing, and reduces pain, through the modulation of cellular and molecular pathways [10]. PBMT-treated ischemic tissues demonstrated enhanced angiogenesis and nitric oxide release as well as an increase in cells expressing Vascular Endothelial Growth Factor (VEGF) Hypoxia-Inducible Factor alpha (HIF-1) [11-13]. In addition, PBMT can improve flap survival by increasing the number of new blood vessels growing in tissues, altering VEGF release, stimulating matrix metalloproteinase-2 (MMP,-2) expressing the presence of HIF-1 [14].
It has recently been demonstrated that PBMT and stem cells can speed up the healing of diabetic-infected types one and two wounds in rats [15-17]. Therefore, previous related studies have demonstrated that the simultaneous use of the two treatment modalities is beneficial for the treatment of serious diseases such as severe cases of DFU. They can be addictive and are an advanced treatment for DFU [17,18].
Recently introduced a flexible methacrylate dressing (Altrazeal powder) [19]. A dressing made of methacrylate has been used to treat surgical wounds and wounds that take a long time to heal, vascular limb ulcers, edematous ulcers [19], refractory venous leg ulcers [20], and patients with chronic leg ulcers. The powder, when applied to the exudate wound, will interact with moisture, agglomerate, and form a porous, fast-healing surface environment [20]. When used for diabetic foot, this therapy has been shown to be effective [19] and burn patients’ skin graft donor sites. Using this dressing has also been reported to improve infection control [21].
In the current study, we investigated the mixed impact of the Altrazeal powder with PBMT on the healing of a complicated case of DFU and CFU number in a 55 years old man with type one DM, unable to respond to routine treatments and at risk of having foot amputated.
Case presentation
55-year-old man (addicted, heavily smoked) who suffered from type one DM and heart failure has been admitted to the ZAKHM NOOR outpatient clinic. He had an extensive 37 cm2 full-thickness cutaneous wound in the plantar part of his right foot (Wagner Ulcer Grade Classification System: grade 3) (Figure 1) that have previously undergone unsuccessful standard of care wound therapy. During clinical examination, it was observed considerable colliquative necrosis of the soft tissues and discharge of pus in the ulcer. The biochemical data revealed an acute leukocytosis with a WBC count of 22x109 cells per liter, blood sugar levels >320 mg/dl, and an HgBA1C of 12%.
Microbial sampling was done in the first and last session of treatment (Mueller-Hinton agar) (Figures 2 & 3).
PBMT was used once a week for 20 weeks and performed 37 shootings of the laser over the ulcer surface and adjacent to normal skin in each session and finally the wound was constricted (Figure 4). According to the following protocol and guideline, which is listed in Table 1, we used the Novin Tech laser machine (Novin Tech Co., Iran).
After PBMT, Altrazeal powder was topically used to supply moisture control, decrease the need for dressing changes, and stimulate the wound healing process. The powder was applied with drops of saline on the surface of the ulcer. And ulcer was dressed with Vaseline dressing. Afterward, the offloading bandage was applied to relieve pressure from the weight-bearing portion of the foot, and dressing changes were made over weekly intervals.
Table 1: The course of endoscopic treatments.
| Mode | Pulsed |
|---|---|
| PeakPower (mW) | 1000 |
| AveragePower (mW) | 400 |
| Theenergy density (J/cm2) | 3 |
| Frequency(number) | 10000 |
| Wavelength(nm) | 870 |
| Exposuretime per point(s) | 6 |
| Spotarea (cm2) | 1 |
| Numberof points | 37 |


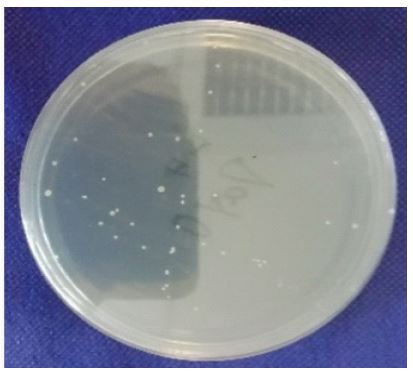

Table 2: Assessment of VAS pain levels during the follow-up period.
| Week 1 | Week 6 | Week 12 | Week 20 |
|---|---|---|---|
| 7 | 5 | 3 | 0 |
Every week, the clinical condition was assessed, which indicated a decrease in the ulcer size, pain, and reduced inflammatory reaction, along with more structured tissue formation, hemostasis, and remarkable coagulation. The absolute remission of the lesions with a high level of healthy skin was the 20th week of follow-up’s most beneficial aspects. And absence of pain analyzed by the Visual Analogue Scale (VAS) in Table 2.
Discussion
Under typical conditions, inflammatory phase of wound healing process is correlated, lasting only a few days, and the healing phases progress normally [4]. However, in DM, the inflammatory phase lasts longer and the entire damaged skin does not heal, resulting in slow healing [22]. Patients with DFU endure a variety of treatments throughout their lives, which are costly and place a significant financial strain on communities and insurance organizations [1,23]. The cost of chronic wound care has increased as the population ages and the number of diabetics increases. New treatment procedures that improve patients’ ability to cope will benefit them [24,25].
The current case study reveals a special and complementing approach in which both modalities (Altrazel dressing and PBMT) were chosen to promote healing and provide patient comfort. Reduces healing time of ulcerated areas.
Present day, nano science plays an essential role in promoting wound healing. Altrazeal uses nanoparticles that can be modified to give the best-wound dressing. This sterile mixture of 85% poly-2-Hydroxyethyl Methacrylate (pHEMA) and 15% poly-2-hydroxypropyl methacrylate (pHPMA) is suitable for opoperative wounds, acute peripheral leak wounds, including grafts of donor and second-degree burns, as well as chronic wounds, slow-healing sores [26]. When the sterile nanoparticle powder is put on a wet injury bed, it joins with ionized liquids like exudate, saline, or blood to shape a clustered, exudate-controlling injury dressing. The flexible wound gauze adjusts to the region of the injury bed once amassed, filling vulnerable sides and containing wound edges. The permeable construction of the polymer produced by actuation takes into account superb oxygen and fume happening, immovability, and consistency, all of which help to safeguard the injury during healing [19]. This dressing also assists to seal the wound margins and this is a bacteria-resistant, reducing the possibility of additional bacterial contamination [19].
In consumed wounds, it was also proposed to use pHEMA in conjunction with various admixtures, such as polyethylene glycol-400 (PEG), including antimicrobial added substances like silver sulfadiazine, silver nitrate, gentamicin, or nitrofurazone [27]. Studies show adding the antimicrobial compounds to a pHEMA base reduce the number of bacteria in burn wounds and relieved pain in patients, according to experimental and clinical studies [28,29]. PBMT has an inhibitory impact on S. aureus growth by stimulation of ROS (Reactive Oxygen Species) synthesis. consistent with this finding, the combination of the PBMT and Altrazeal have synergic impacts in reduction of CFU number in the wound.
It appears to be stimulating a variety of cell types and actions, particularly in the wound bed, and angiogenesis was the focus of PBMT [6]. PBMT is also a non-interfering treatment that relieves pain through analgesic and anti-inflammatory effects [30,31]. The release of neurochemical agents like endogenous endorphins (-endorphin), a reduction in C-fiber and bradykinin activity under the influence of PBMT, and a shift in pain threshold are thought to be some of the factors that contribute to the analgesic effect [31,32]. In the past and current studies, the patient’s pain decreased during therapy and was analyzed by the VAS method [32]. PBMT can also stimulate the growth of epithelial, endothelial, and mesenchymal cells while also increasing tissue oxygenation and microcirculation [33].
Our limitation in the study: The 3D camera was not available, so the depth of the wound was not evaluated.
Conclusion
The positive impact that the mixture of photobiomodulation therapy and Altrazeal wound dressing had on the colony-forming unit of a diabetic foot ulcer was demonstrated in this present case report. To validate our results, further clinical trials are suggested. moreover, it is recommended that additional research using preclinical models uncover the mechanism of action of the combination of PBMT and Altrazeal powder.
Declarations
Competing interests: The authors declare that they have no competing interests.
Availability of data and material: Not applicable.
Authors contributions: EM, LAY collected patient data, HA wrote the manuscript.
Consent to publication: The patient gave written informed consent to publish this manuscript.
References
- Mostafavinia A, Ahmadi H, Amini A, Roudafshani Z, Hamblin MR, et al. The effect of photobiomodulation therapy on antioxidants and oxidative stress profiles of adipose derived mesenchymal stem cells in diabetic rats. Spectrochimica Acta Part A: Molecular and Biomolecular Spectroscopy. 2021; 262: 120157.
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes research and clinical practice. 2019; 157: 107843.
- Dalla Paola L. Diabetic foot wounds: The value of negative pressure wound therapy with instillation. International wound journal. 2013; 10 Suppl 1(Suppl 1): 25-31.
- Mostafavinia A, Amini A, Sajadi E, Ahmadi H, Rezaei F, et al. Photobiomodulation therapy was more effective than photobiomodulation plus arginine on accelerating wound healing in an animal model of delayed healing wound. Lasers in Medical Science. 2022; 1-13.
- Nikoloudi M, Eleftheriadou I, Tentolouris A, Kosta OA, Tentolouris N. Diabetic foot infections: update on management. Current infectious disease reports. 2018; 20(10): 1-11.
- Ahmadi H, Bayat M, Amini A, Mostafavinia A, Ebrahimpour-Malekshah R, et al. Impact of preconditioned diabetic stem cells and photobiomodulation on quantity and degranulation of mast cells in a delayed healing wound simulation in type one diabetic rats. Lasers in Medical Science. 2022; 37(3): 1593-604.
- Lipsky BA. Diabetic foot infections: Current treatment and delaying the ‘post‐antibiotic era’. Diabetes/metabolism research and reviews. 2016; 32: 246-53.
- Schreiber AK, Nones CF, Reis RC, Chichorro JG, Cunha JM. Diabetic neuropathic pain: Physiopathology and treatment. World journal of diabetes. 2015; 6(3): 432.
- Jeffcoate WJ, Vileikyte L, Boyko EJ, Armstrong DG, Boulton AJ. Current challenges and opportunities in the prevention and management of diabetic foot ulcers. Diabetes care. 2018; 41(4): 645-52.
- Mostafavinia A, Amini A, Sajadi E, Ahmadi H, Rezaei F, et al. Photobiomodulation therapy was more effective than photobiomodulation plus arginine on accelerating wound healing in an animal model of delayed healing wound. Lasers in Medical Science. 2022; 37(1): 403-15.
- Mostafavinia A, Amini A, Ahmadi H, Rezaei F, Ghoreishi SK, et al. Combined Treatment of Photobiomodulation and Arginine on Chronic Wound Healing in an Animal Model. Journal of Lasers in Medical Sciences. 2021; 12.
- Ma J-X, Yang Q-M, Xia Y-C, Zhang W-G, Nie F-F. Effect of 810 nm near-infrared laser on revascularization of ischemic flaps in rats. Photomedicine and Laser Surgery. 2018; 36(6): 290-7.
- Martignago C, Tim C, Assis L, Andrade A, Brassolati P, et al. Preemptive treatment with photobiomodulation therapy in skin flap viability. Journal of Photochemistry and Photobiology B: Biology. 2019; 201: 111634.
- Cury V, Moretti AIS, Assis L, Bossini P, De Souza Crusca J, et al. Low level laser therapy increases angiogenesis in a model of ischemic skin flap in rats mediated by VEGF, HIF-1α and MMP-2. Journal of Photochemistry and Photobiology B: Biology. 2013; 125: 164-70.
- Ahmadi H, Amini A, Fadaei Fathabady F, Mostafavinia A, et al. Transplantation of photobiomodulation-preconditioned diabetic stem cells accelerates ischemic wound healing in diabetic rats. Stem cell research & therapy. 2020; 11(1): 1-14.
- Ebrahimpour-Malekshah R, Amini A, Zare F, Mostafavinia A, Davoody S, et al. Combined therapy of photobiomodulation and adipose-derived stem cells synergistically improve healing in an ischemic, infected and delayed healing wound model in rats with type 1 diabetes mellitus. BMJ Open Diabetes Research and Care. 2020; 8(1): e001033.
- Moradi A, Zare F, Mostafavinia A, Safaju S, Shahbazi A, et al. Photobiomodulation plus adipose-derived stem cells improve healing of ischemic infected wounds in type 2 diabetic rats. Scientific reports. 2020; 10(1): 1-15.
- Amini A, Soleimani H, Abdollhifar MA, Moradi A, Ghoreishi SK, et al. Stereological and gene expression examinations on the combined effects of photobiomodulation and curcumin on wound healing in type one diabetic rats. Journal of cellular biochemistry. 2019; 120(10): 17994-8004.
- Fitzgerald RH, Bharara M, Mills JL, Armstrong DG. Use of a Nanoflex powder dressing for wound management following debridement for necrotising fasciitis in the diabetic foot. International wound journal. 2009; 6(2): 133-9.
- Carretero RG, Garrido-Ollero M, Martinez-Alvarez A, Cadenas-Vara A. Methacrylate dressing on refractory venous leg ulcers. Case Reports. 2018; 2018: bcr-2017-223084.
- Assadian O, Arnoldo B, Purdue G, Burris A, Skrinjar E, et al. A prospective, randomised study of a novel transforming methacrylate dressing compared with a silver‐containing sodium carboxymethylcellulose dressing on partial‐thickness skin graft donor sites in burn patients. International wound journal. 2015; 12(3): 351-6.
- Cañedo-Dorantes L, Cañedo-Ayala M. Skin acute wound healing: A comprehensive review. International journal of inflammation. 2019; 2019.
- Chouhan D, Dey N, Bhardwaj N, Mandal BB. Emerging and innovative approaches for wound healing and skin regeneration: Current status and advances. Biomaterials. 2019; 216: 119267.
- Coalson E, Bishop E, Liu W, Feng Y, Spezia M, et al. Stem cell therapy for chronic skin wounds in the era of personalized medicine: From bench to bedside. Genes & diseases. 2019; 6(4): 342-58.
- Tamama K, Kerpedjieva SS. Acceleration of wound healing by multiple growth factors and cytokines secreted from multipotential stromal cells/mesenchymal stem cells. Advances in wound care. 2012; 1(4): 177-82.
- St John J, Brown S, Hatef D, Unzeitig A, Noble D, et al. Formulation development and in vivo testing of a novel powder wound dressing employing dehydrated hydrogel nanoparticle technology. The University of Texas Southwestern Medical Center at Dallas, Department of Plastic Surgery. 1801.
- Nathan P, Robb EC, Law EJ, MacMillan BG. A clinical study of antimicrobial agents delivered to burn wounds from a drug-loaded synthetic dressing. The Journal of Trauma. 1982; 22(12): 1015-8.
- Fang C, Nathan P, Robb EC, Alexander JW, MacMillan BG. Prospective clinical study of Hydron, a synthetic dressing, in delivery of an antimicrobial drug to second-degree burns. The Journal of Burn Care & Rehabilitation. 1987; 8(3): 206-9.
- Deitch EA, Sittig K, Heimbach D, Jordan M, Cruse W, et al. Results of a multicenter outpatient burn study on the safety and efficacy of Dimac-SSD, a new delivery system for silver sulfadiazine. The Journal of trauma. 1989; 29(4): 430-4.
- Silveira PCL, Silva LA, Freitas TP, Latini A, Pinho RA. Effects of low-power laser irradiation (LPLI) at different wavelengths and doses on oxidative stress and fibrogenesis parameters in an animal model of wound healing. Lasers in medical science. 2011; 26(1): 125-31.
- Andrade FdSdSD, Clark RMdO, Ferreira ML. Effects of low-level laser therapy on wound healing. Revista do Colégio Brasileiro de Cirurgiões. 2014; 41: 129-33.
- Derakhshan R, Ahmadi H, Bayat M, Pourhashemi E, Amini A, et al. The Combined Effects of a Methacrylate Powder Dressing (Altrazeal Powder) and Photobiomodulation Therapy on the Healing of a Severe Diabetic Foot Ulcer in a Diabetic Patient: A Case Report. Journal of Lasers in Medical Sciences. 2022; 13: e38-e.
- Hagiwara S, Iwasaka H, Okuda K, Noguchi T. GaAlAs (830 nm) low‐level laser enhances peripheral endogenous opioid analgesia in rats. Lasers in Surgery and Medicine: The Official Journal of the American Society for Laser Medicine and Surgery. 2007; 39(10): 797-802.