
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Anal fistulas at roof of ischiorectal fossa inside levator ani muscle (RIFIL): MRI’s key role their management
Halfi Mohamed Ismail*; Benmoussa Meriem; Laamrani Fatima Zahra; Jroundi Laila
Department of Emergency Radiology, Ibn Sina University Hospital Center, Rabat, Morocco.
*Corresponding Author : Halfi Mohamed Ismail
Department of Emergency Radiology, Ibn Sina University Hospital Center, Rabat, Morocco.
Email: ismail.m.halfi@gmail.com
Received : May 01, 2024
Accepted : May 21, 2024
Published : May 28, 2024
Archived : www.jcimcr.org
Copyright : © Ismail HM (2024).
Citation: Ismail HM, Meriem B, Zahra LF, Laila J. Anal fistulas at roof of ischiorectal fossa inside levator ani muscle (RIFIL): MRI’s key role their management. J Clin Images Med Case Rep. 2024; 5(5): 3079.
Description
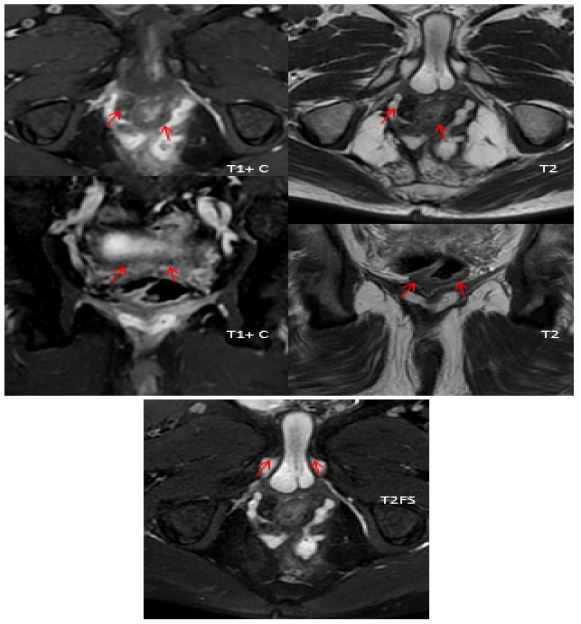
Fistulas pathways in the anal and rectal region are tricky to delimit and define their extension using imaging (MRI) because of the multilayer and condense anatomy of this region. Recently, with the increased clarity that MRIs brought to this pathology, 5 fistula pathways has been diagnosed known as peri-levator high-5 anal fistulas: Supralevator, suprasphincteric, extrasphincteric, high intrarectal fistulas and high outersphincteric [2]. In the latter, a fistula at the roof of ischiorectal fossa inside the levator ani muscle (RIFIL), has been described. The fistulas do not cross the sphincter as they remain in the heart of the leavtor muscle and do not enter the ischiorectal fossa. A retrospective study analysing 419 operated fistula patients: 10% had RIFIL and the rest non-RIFIL fistuals. Main points of comparasing is that the RIFIL fistuals group were more recurrent, with multiple more complex and ambiguous tracts consequently the surgery failure rate was significantly higher in the RIFIL group (30.6%) than in the non-RIFIL fistula (7.2%) [1]. Clinically, due to their deep and elevated anatomical topography, they are almost impossible to diagnose on clinical examination. Using MRI or Transrectal ultrasound, we can effectively and accurately study their internal opening, primary tracts and secondary extensions. Therefore, MRI is considered mandatory to diagnose these fistulas, their side branch in case of multiple recurrences as well as the efficacy post operatively. Transanal Opening of Intersphincteric Space (TROPIS) has an average successful rate with minimal impact on continence in RIFIL fistulas, because the surgical accessibility to the RIFIL is difficult. The ligation of the intersphincteric fistula tract LIFT and Fistula Repair Procedure (FPR) predicted to achieve a moderate level of success. Nevertheless, there haven’t been any studies conducted on the use of LIFT or FPR procedures specifically for RIFIL fistulas, which have been recently described [2]. Care should be taken to always favour and proceed with sphincter-sparing approaches such as TROPIS or LIFT. This is the case of 45-year-old male patient with inflammatory Bowel Disease and had a Seton drain placed for a anal fistula. Despite the drain anal discharge stayed active. MRI showed a complex fistulous trajectory in the outer high outersphincteric space, an entry orifice at 6 o’clock with wide infected paths and an exit orifice at the level of the right inter gluteal fold. The patient underwent a LIFT procedure with a lavage of the abcesses with a good post-operative outcome. Overall, it is very important to avoid missing the diagnosis of RIFIL fistula s otherwise the recurrent rate would remain high. These have not been described previously and are perhaps confused with high transsphincteric infralevator fistulas in ischiorectal fossa [1,2].
Horseshoe intersphincter course
Posterior transphincter supplying an abscessed collection at 5 o clock
Transphincterian at 7 o’clock
Tran sphincter at 9 o’clock descending to the level of the right ischio anal fossa.
References
- Garg P, Dawka S, Yagnik VD, Kaur B, Menon GR. Anal fistula at roof of ischiorectal fossa inside levator-ani muscle (RIFIL): A new highly complex anal fistula diagnosed on MRI. Abdom Radiol (NY). 2021; 46(12): 5550-5563.
- Garg P, Yagnik VD, Dawka S, Kaur B, Menon GR. Guidelines to diagnose and treat peri-levator high-5 anal fistulas: Supralevator, suprasphincteric, extrasphincteric, high outersphincteric, and high intrarectal fistulas. World J Gastroenterol. 2022; 28(16): 1608-1624.