
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Case report: A seldom-seen instance of a massive spigelian hernia with huge hernial sac
*Corresponding Author : Sneha KR
Akash Institute of Medical Sciences and Research Centre, Devanahalli, Rural Bangalore, India.
Email: drsnehaakr@gmail.comg
Received : May 20, 2024
Accepted : Jun 04, 2024
Published : Jun 11, 2024
Archived : www.jcimcr.org
Copyright : © Sneha KR (2024).
Abstract
Introduction and importance: Spigelian hernias, rare defects in the abdominal wall, manifest at the semilunar line lateral to the rectus abdominis muscle. Situated amidst the muscular layers of the abdominal wall, they may escape detection due to abdominal obesity. Diagnosis proves challenging due to their location and nonspecific symptoms. However, ultrasonography and Computed Tomography have significantly improved diagnostic accuracy.
Clinical discussion: Spigelian hernias make up approximately 0.12 to 0.2% of all abdominal hernias. They typically manifest along the semilunar line, characterized by a distinct defect in the Spigelian aponeurosis known as the “Spigelian hernia” belt. Ultrasound scanning is advised as the initial imaging investigation in suspected cases. Prompt surgical repair is recommended for Spigelian hernias to avert potential strangulation.
Conclusion: Given the rarity of Spigelian hernias, a heightened level of suspicion is crucial for accurate diagnosis. Upon confirmation of the diagnosis, operative intervention is necessary to prevent the possibility of incarceration.
Citation: Sneha KR. Case report: A seldom-seen instance of a massive spigelian hernia with huge hernial sac. J Clin Images Med Case Rep. 2024; 5(6): 3109.
Introduction and importance
The initial clinical depiction of a hernia forming along the Spigelian line was documented by Klinkosch [1]. The Belgian anatomist Adriaan van der Spieghel (Adrianus Spigelius) was the first to delineate the crescent line now recognized as the Spigelian line in 1645 [2]. These hernias are infrequent, constituting 1 to 2% of all abdominal wall hernias [1].
The segment of the transversus abdominis aponeurosis situated between the lateral semilunar line and the lateral border of the medial rectus muscle is termed the Spigelian aponeurosis. Spigelian hernias are located between the layers of abdominal muscles along the semilunar line and are referred to as lateral ventral, interparietal, intermuscular, or intramural hernias. Although they maintain a specific position along the semilunar line (Spieghel), they are termed “interstitial hernias” and should be distinguished from other types of interstitial hernias. Most of these hernias occur in the lower abdomen, where the posterior sheath is deficient. The hernia ring presents as a well-defined defect in the transverse aponeurosis [3]. Factors that contribute to increased tension on the abdominal wall aponeurosis or heightened intra-abdominal pressure, such as straining due to bladder outlet obstruction, chronic cough, obesity, or multiple pregnancies, are believed to be risk factors for the development of Spigelian hernias [4]. Diagnosing Spigelian hernias can be challenging due to their concealment by abdominal fat and the aponeurosis of the external oblique. The fascial margin around the defect is sharp, increasing the risk of strangulation and incarceration, estimated at about 24%. Consequently, surgical intervention is often recommended, typically performed via traditional open approach with primary suture repair or by utilizing an onlay or sublay mesh technique [5]. This study adheres to the SCARE criteria for reporting surgical case reports [6].
Case presentation
A 42 years female presented to the general surgery outpatient department with complaints of swelling in the left lumbar region of the abdomen since 10 days. Swelling was associated with pain since 10 days.
Clinical case discussion
Patient was apparently normal 10 days back, then noticed swelling in left lumbar region of abdomen, swelling was insidious in onset, non progressive, reduced on lying down and increased on working. Associated with abdominal pain, dull aching type in left lumbar region- non radiating type without any features of intestinal obstruction like severe abdominal pain and vomiting. She is a known Hypothyroidism for 5 years on medical thyronorm 150 mcg and no other Co-morbidities present. She was diagnosed right latero ventral hernia 8 years back for which she has undergone hernia mesh repair. She also was later diagnosed with right strangulated ventral hernia 3 years back and was operated for same.
On examination soft swelling of size 10 x 10 cm was palpable in the left lumbar region of abdomen, well defined and increases on coughing (Figure 1).

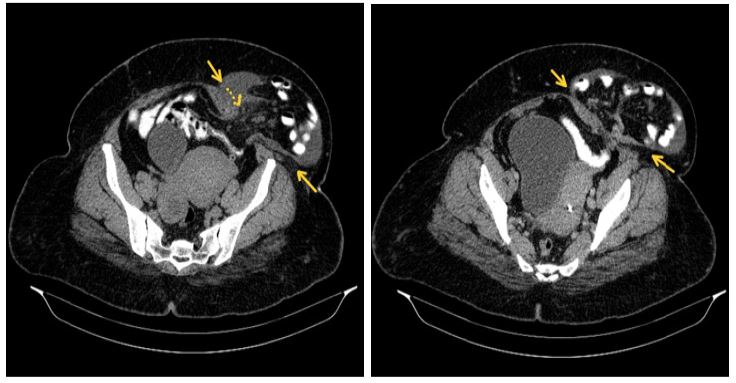
Patient was advised for Ultrasonography, where impression was given as ventral hernia. How ever patient was further investigated with contrast enhanced CT scan (Figure 2) in which the following observation was made, a defect measuring 5x5 cm in the anterior abdominal wall between left rectus muscle and rest of the abdominal wall muscles along the semilunar line. Distal ileal loops are seen herniating through this defect in transverses abdominus aponeurosis into the subcutaneous plane. Minimal free fluid is noted within the hernia sac and in the mesentery. There is no abnormal bowel dilatation/ bowel wall thickening / small bowel feces sign. Linear scar noted in the anterior abdominal wall to the right between right rectus and rest of the abdominal wall muscles.
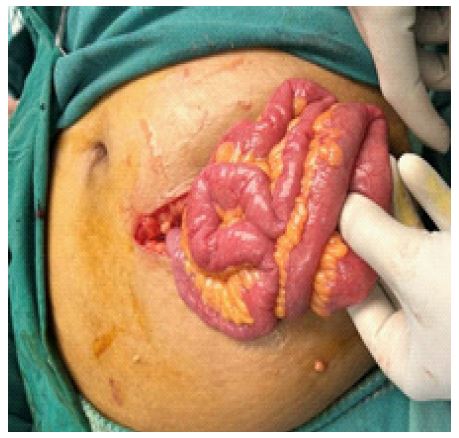
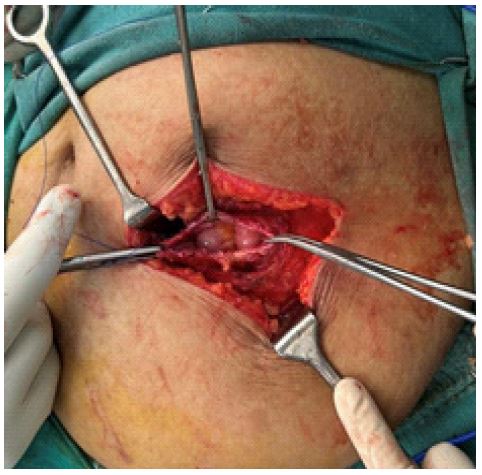
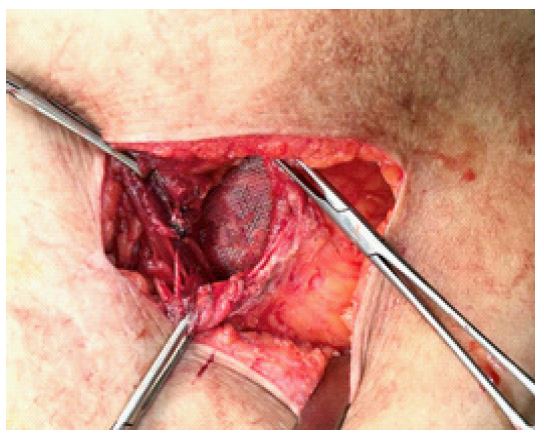
Fluid density lesion at the umbilicus approximately measuring 44x2.2 cm with small intraperitoneal extension and impression give was Left Spigelian hernia with signs of impending bowel strangulation. Preoperative preparation was done and the patient underwent Open mesh Hernioplasty under spinal anesthesia. Patient was supine positioned, Transverse incision was made in the left lumbar region, sac was identified which was approximately measuring about 10x10 cm (Figure 3), structures around the sac dissected and incision was made in the sac and fluid drained with suction. Content was bowel and defect (Figure 4) was 5x5 cm in size (Figure 5). Defect was extended and the contents were pushed into the peritoneum and peritoneum was closed. Sac was excised and plane was made around the defect, Mesh measuring 7x15 cm was placed (Figure 6). Mesh was secured with proline suture material and drain was placed, other drain was placed in subcutaneous space as well, all the layers of abdomen was closed layer by layer. Skin was closed with Ethilone.

Patient was under observation at hospital for 5 days, had no complaints. Drains were removed and was discharged on 5th postoperative day without any complications. Patient was advised to avoid strenuous activity. She was on regular follow up for 5 months. She is healthy at present and happily living.
Discussion
Spigelian hernias, also known as “spontaneous lateral ventral hernias” or “hernias of the semilunar line,” are rare inter-parietal hernias. Sometimes referred to as intraparietal, interstitial, intramuscular, or intramural hernias, they are situated between different muscle layers of the abdominal wall [3]. The “Spigelian hernia belt,” located in a paramedian region 0 to 6 cm cranial to a line running between both anterior superior iliac spines, is where Spigelian hernias primarily occur [7]. The Spigelian fascia widens along the semilunar line, especially as it nears the umbilicus [3].
The hernia sac, enveloped by extra-peritoneal fatty tissue, typically traverses the transverse and internal oblique aponeurosis and spreads behind the intact aponeurosis of the external oblique [3]. Although the hernia sac usually contains the greater omentum, other organs, such as the small intestine, colon, stomach, gallbladder, Meckel’s diverticulum, appendix, ovaries and testes, may be involved [7].
Diagnosing Spigelian hernias preoperatively is often challenging due to the atypical clinical symptoms and lack of personal clinical experience with Spigelian defects [8]. While history and physical examination are relied upon in many cases, patients who undergo CT or Ultrasound imaging potentially provide diagnostic assistance [7]. The differential diagnosis includes rectus sheath hematoma, abdominal wall abscess, and seroma [8].
Surgical intervention is the standard management for Spigelian hernias, typically performed using either open or laparoscopic techniques. Laparoscopic repair is associated with a lower recurrence rate, decreased morbidity, and shorter hospital stay [9]. In the case of our patient, an open approach provided optimal exposure in a timely manner.
Conclusion
Spigelian hernias are rare multifactorial disorders characterized by a defect in the transversus abdominis muscle in the anterior abdominal wall, resulting in the protrusion of visceral content through the hernia defect. These hernias pose a significant risk of incarceration and strangulation of their contents. Clinical presentation is often nonspecific, leading to dilemma in: diagnosis. Physical examination, coupled with CT scan, is the most definitive radiologic test for establishing a diagnosis of Spigelian hernia. Surgical intervention is always necessary for managing Spigelian hernias, which can be performed in a traditional open manner or laparoscopically, with a low recurrence rate following surgical repair.
Declarations
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval: Ethical approval is exempt at our institute.
Funding: none.
References
- Angel Celdr´an, et al., The open mesh repair of Spigelian hernia, Am. J. Surg. 2007; 193(1): 111-113.
- Beart Jr, Robert W., et al. “AMERICAN*** SURC, E ( ) N”.
- Hemant Panditrao Mhatre, Vijay Bhaskarrao Kanake, Vipul Versi Nandu, Spigelian hernia: a rare case presentation, Int. Surg J. 2015; 2(4): 717-720.
- PO Igwe, NA Ibrahim, Strangulated sliding spigelian hernia: a case report, Int. J Surg. Case Rep. 2018; 53: 475-478.
- Adeline Rankin, Milo Kostusiak, Ashraf Sokker, Spigelian hernia: case series and review of the literature, Visceral Med. 2019; 35(2): 133-136.
- RA Agha, T Franchi, C Sohrab, G Mathew, A Kirwan, A Thomas, et al. The SCARE 2020 guideline: Updating consensus Surgical Case Report (SCARE) guidelines, Int. J. Surg. 2020; 84(1): 226-230.
- David W. Larson, David R. Farley, Spigelian hernias: repair and outcome for 81 patients, World J. Surg. 2002; 26: 1277-1281.
- Wael Zaki, Awad Ali M. Alawad, Spigelian hernia: a rare case report, Ann. Clin. Case Rep. 2017; 2.
- Saad Slaiki, et al. Spigelian hernia case report and review of literature, Int. Surg J. 2020; 7(3): 880-882.