
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Significant hemorrhage following computed tomography- guided fine-needle aspiration biopsy of pancreatic incidentaloma: A case report and literature review
Athena Myrou1*; Georgia Kaiafa2; Stavros Savvakis1; Afroditi Dristela1; Panagiotis-Konstantinos Emfietzis1; Christos Savopoulos1
1First Propaedeutic Department of Internal Medicine, General University Hospital AHEPA, Thessaloniki, Greece.
2Department of Haematology, First Propaedeutic Department of Internal Medicine, General University Hospital AHEPA, Thessaloniki, Greece.
*Corresponding Author : Athena Myrou
First Propaedeutic Department of Internal Medicine, General University Hospital AHEPA, Thessaloniki, Greece.
Tel: +306949867515.
Email: taniamyrou@gmail.com
Received : Jun 28, 2024
Accepted : Aug 22, 2024
Published : Aug 29, 2024
Archived : www.jcimcr.org
Copyright : © Myrou A (2024).
Abstract
Pancreatic incidentalomas are asymptomatic pancreatic lesions detected by imaging procedures conducted for purposes unrelated to the original diagnostic inquiry. The prevalence of these lesions has increased with advancements in imaging technologies. Determining the malignant potential of pancreatic incidentalomas is crucial. Histological confirmation through Fine-Needle Aspiration (FNA) biopsy is often required to guide treatment decisions. This case report presented a 78-year-old male patient who underwent Computed Tomography (CT)-guided FNA biopsy of a pancreatic incidentaloma located at the tail of the pancreas. The patient experienced significant hemorrhage following the procedure, as evidenced by a decline in hemoglobin levels despite transfusion. CT angiography revealed a perisplenic and perihepatic fluid collection extending into the right paracolic gutter and pelvis. Surgical assessment and splenic artery embolization were performed to manage the hemorrhage. The patient recovered without any further complications and was discharged. A literature review of complications associated with CT-guided pancreatic FNA biopsy yielded limited data, with most studies reporting minor bleeding. This case highlighted the potential for significant hemorrhage following CT-guided FNA biopsy of pancreatic incidentalomas and emphasized the importance of prompt recognition and management to ensure patient safety and optimal outcomes.
Keywords: Pancreatic incidentalomas; Hemorrhage; Computed tomography; Fine-needle aspiration; Pancreatic neoplasms.
Abbreviations: FNA: Fine-Needle Aspiration; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; DSA: Digital Subtraction Angiography.
Citation: Myrou A, Kaiafa G, Savvakis S, Dristela A, Emfietzis PK, et al. Significant hemorrhage following computed tomography-guided fine-needle aspiration biopsy of pancreatic incidentaloma: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(8): 3228.
Introduction
Impressive progress in imaging technology has led to the incidental discovery of asymptomatic pancreatic lesions. These lesions are detected by imaging procedures conducted for reasons unrelated to the pancreas and have been named pancreatic incidentalomas [1,2]. Histologically, pancreatic incidentalomas represent a variety of pathological entities ranging from small cysts to large invasive pancreatic tumors. According to a retrospective review by Spinelli et al. [4], incidental pancreatic cysts were identified in 1.2% of 24,039 patients who underwent abdominal imaging [3]. A recent retrospective study using high-resolution magnetic resonance imaging identified asymptomatic pancreatic cysts in 9.3% of patients.
The initial concern after detection of a pancreatic incidentaloma is whether the lesion is malignant; consequently, further diagnostic workups are required. Although the indications for biopsy of suspected malignant incidental lesions are still controversial, it is widely accepted that histological confirmation is essential when it may crucially influence treatment decisions [5]. The predominant method for tissue acquisition from a pancreatic mass is Fine-Needle Aspiration (FNA) while utilizing Computed Tomography (CT), transabdominal ultrasonography, or endoscopic ultrasound for guidance [6]. These diagnostic approaches are invasive and can be associated with complications.
The current study presented a case involving notable hemorrhage after CT-guided FNA on a pancreatic incidentaloma and the subsequent management of the patient. Additionally, a brief review of the literature was conducted to examine the prevalence of bleeding and other complications arising from pancreatic FNA biopsies with the aim of informing clinical practitioners of their potential occurrence.
Case report
A 78-year-old male was admitted to the Emergency Department with shortness of breath. Past medical history included type 2 diabetes mellitus, pulmonary hypertension, narrowing of the left carotid artery, and prior surgical removal of a colon polyp. Laboratory examination revealed pancytopenia; therefore, the patient was admitted to the hematology department for further investigation. During hospitalization, the patient underwent an osteomyelitis biopsy with immunophenotype, which was negative for any type of hematological disorder. He received one unit of red blood cells and antibiotics and nebulization.
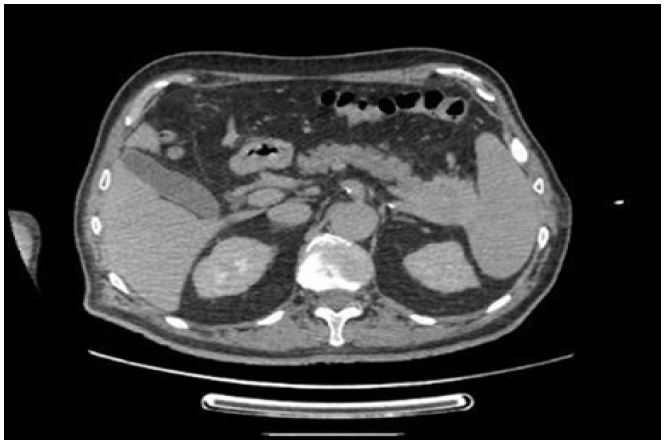
A CT pulmonary angiogram and abdominal CT were performed. The latter revealed a tumor (4.0 cm × 3.3 cm × 5.3 cm, transverse × anteroposterior × cephalic diameter) located at the tail of the pancreas. It was in direct contact with the spleen and the anterior perirenal fascia (Figure 1). The pancreatic mass infiltrated the splenic vein while encasing the splenic artery at the same level. Abdominal magnetic resonance imaging was also performed. It revealed that the tumor (5.1 cm × 4.0 cm × 5.4 cm, anteroposterior × transverse × cephalic diameter) infiltrated the spleen and the splenic vein, and there was a pathological lymph node approximately 1 cm from the tumor (Figure 2).
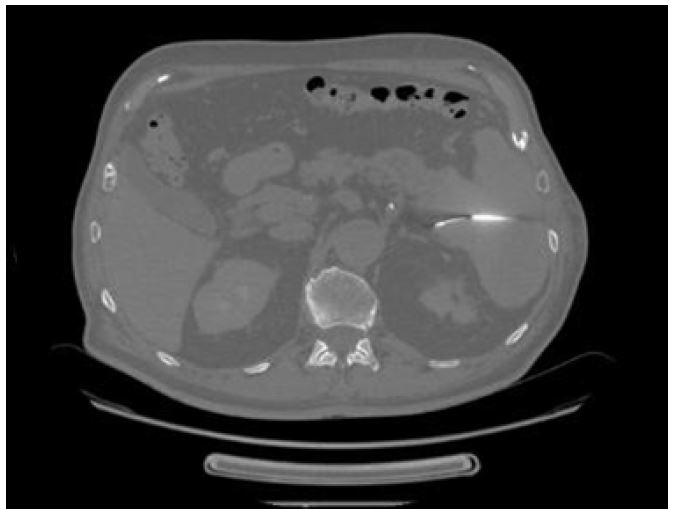
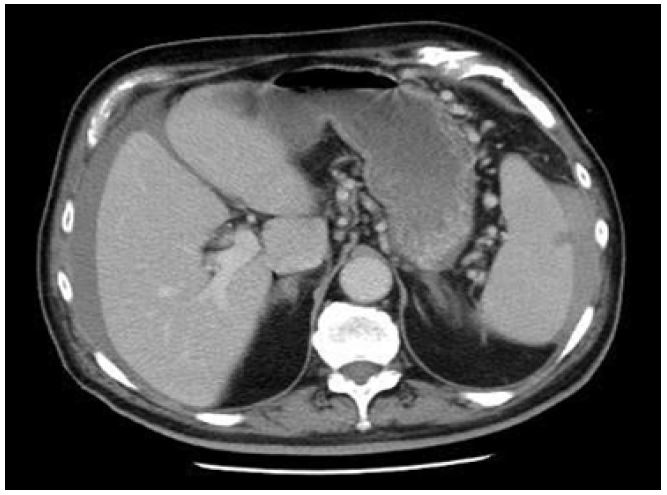
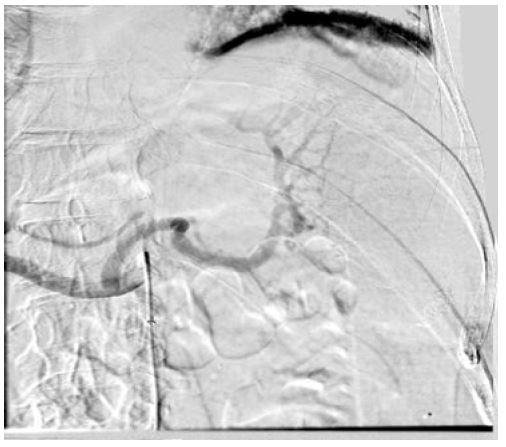
The patient was scheduled for FNA biopsy of the tumor. FNA biopsy was performed on June 27, 2023 (Figures 3 and 4), and the patient was hospitalized for 24 hours for monitoring. Laboratory examination on June 28, 2023 showed a 2 g/dL drop in hemoglobin (pre-biopsy: 10.1 g/dL, post-biopsy: 7.8 g/dL). The patient was hemodynamically stable and received with one unit of red blood cells. Despite the transfusion, there was no improvement, with the hemoglobin level at 8.1 g/dL on June 29, 2023. CT angiogram was performed and showed no sign of active extravasation. However, a perisplenic and perihepatic collection of fluid (hemorrhagic) that was distributed at the right paracolic gutter and pelvis was revealed. Surgical assessment, splenic artery embolization, and transfusion of two units of red blood cells and two units of fresh frozen plasma were performed. Embolization was performed on June 30, 2023 through the right profunda femoris artery under ultrasound guidance using a Cobra catheter and a Progreat microcatheter. The splenic artery was catheterized and embolized using multiple coils and a hemostatic sponge. There were no intraoperative or postoperative complications, and the patient was discharged on July 7, 2023. The dyspnea initially experienced by the patient was associated with pulmonary hypertension. Pulmonary embolism and other acute causes of dyspnea were excluded.


Discussion
Percutaneous FNA biopsy of pancreatic lesions under CT guidance is a minimally invasive, outpatient technique that does not require general anesthesia or sedation [7]. Nevertheless, a certain degree of complications may occur due to the invasive nature of the procedure. Because of the deep retroperitoneal location of the pancreas, establishing a safe route can be challenging. Hemorrhage is the primary concern when puncturing the liver or spleen [8]. Occasionally, interposed blood vessels or collateral vessels may be found along the intended path of the needle. This can lead to varying degrees of hemorrhage with corresponding clinical consequences [9]. In this case, the intervention elicited significant hemoperitoneum. The probable cause was attributed to an injury of the collateral branch of the splenic vessels. Blood originated from the perisplenic area and the omental bursa, which subsequently translocated into the subhepatic space before descending through the right paracolic gutter into the pelvic region. This is in accordance with the anatomical arrangement of the peritoneal cavity [10]. The lone indicator of hemorrhage in our patient manifested as declining hemoglobin levels, which persisted despite transfusion. Although clinical examination revealed normal vital signs, the decision to perform splenic artery embolization was deemed essential to maintain hemodynamic stability and prevent a further decrease in hemoglobin levels. A review of the literature yielded limited data on complications associated with CT-guided pancreatic FNA biopsy. It is likely that the data is limited because of the multitude of guidance modalities (CT, ultrasound, and endoscopic ultrasound) and needle types (FNA and core biopsy) available. In a retrospective analysis conducted by Gruber-Rouh et al. [11] on CT-guided pancreatic FNA biopsy, focal bleeding was observed in 29.2% of all the cases. However, unlike our case, the hemorrhages were minor, detected directly during the intervention, and did not require additional intervention. Similarly, Sofocleous et al. [12] documented self-limiting and clinically insignificant perilesional bleeding in 14% of patients undergoing the same procedure. Tchercansky et al. [7] likewise documented bleeding associated with this diagnostic intervention in 3.7% of biopsies. The bleeding was not situated within the peritoneal cavity but manifested as abdominal wall hematomas. To the best of our knowledge, this is the first documented instance of clinically significant hemoperitoneum requiring intervention after CT-guided pancreatic FNA biopsy. Lew et al. [13] described a single case of hemoperitoneum in a peritoneal dialysis patient. However, they used endoscopic ultrasound for guidance, and the patient received conservative management for bleeding. A systematic review examining the complications associated with endoscopic ultrasound-guided FNA biopsy of the pancreas revealed that only 0.23% of the large patient population experienced major hemorrhage that necessitated interventions such as red blood cell transfusion, endoscopic procedures, or vascular embolization [14]. Ultimately, major hemorrhagic events appear to occur infrequently in relation to these interventional methods. Gupta et al. [15] created guidelines to categorize complications of pancreatic biopsy as minor and major. Minor complications include mild epigastric pain [7], a small focal hemorrhage during biopsy [11,16], and vasovagal reactions [16,17]. Typically, these complications require overnight observation or no treatment. In addition to significant hemorrhage, major complications include acute pancreatitis [16-20], high fever, infection, abscess formation, or sepsis [21,17], severe abdominal pain [16,17], pancreatic duct leakage [16], and bowel perforation [17]. An interesting complication is peritoneal seeding of cancer cells leading to peritoneal carcinomatosis, which was reported in 16.3% of cases by Micames et al. [22]. Major complications require minor-to-extensive hospitalization for treatment and/or have the potential to cause permanent adverse effects. The overall frequency of complications when performing CT-guided FNA biopsy for pancreatic tumors is estimated to be 3.0-6.7% [7].
Conclusion
Modern imaging technologies can accurately detect incidental asymptomatic pancreatic tumors and aid in biopsy procedures for histological diagnosis. CT-guided FNA biopsy of pancreatic tumors is considered safe with a minimal risk of serious complications. This case demonstrated that significant hemorrhage can occur albeit rarely. This case emphasized the importance of careful post-biopsy clinical examination and laboratory testing for patients undergoing this procedure to avert sequelae.
Declarations
Additional materials: Not included.
Acknowledgements: Not applicable.
Authors’ contributions:
AM: Primary case management, literature review, manuscript preparation.
GK: Primary case management, final review of the manuscript.
SS, AF, P-KE: Literature review and manuscript preparation.
CS: Final review of the manuscript.
All authors read and approved the final manuscript.
Funding: Not applicable.
Availability of supporting data: Not applicable.
Ethical approval and consent to participate: No institutional review board approval required.
Patient’s consent for publication: Provided.
Competing interest: The authors declare that they have no competing interests.
References
- Sachs T, Pratt WB, Callery MP, Vollmer CM Jr. The incidental asymptomatic pancreatic lesion: nuisance or threat? J Gastrointest Surg. 2009; 13(3): 405-15. doi: 10.1007/s11605-008-0788-0. Epub 2009 Jan 8. PMID: 19130153.
- Caban M, Małecka-Wojciesko E. Pancreatic Incidentaloma. J Clin Med. 2022; 11(16): 4648. doi: 10.3390/jcm11164648. PMID: 36012893; PMCID: PMC9409921.
- De Oliveira PB, Puchnick A, Szejnfeld J, Goldman SM. Prevalence of incidental pancreatic cysts on 3 tesla magnetic resonance. PLoS One. 2015; 10(3): 0121317. doi: 10.1371/journal.pone.0121317. PMID: 25798910; PMCID: PMC4370618.
- Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A, Komorowski RA, Wilson SD, Pitt HA. Cystic pancreatic neoplasms: observe or operate. Ann Surg. 2004; 239(5): 651-7,657-9. doi: 10.1097/01.sla.0000124299. 57430.ce. PMID: 15082969; PMCID: PMC1356273.
- Iglesias-Garcia J, Lariño-Noia J, Domínguez- Muñoz JE. When to puncture, when not to puncture: Pancreatic masses. Endosc Ultrasound. 2014; 3: 91-7.
- Brugge WR. Pancreatic fine needle aspiration: to do or not to do? JOP. 2004; 5(4): 282-8. PMID: 15254363.
- Tchercansky A, Fernandez Alberti J, Arrechea Antelo R, Bregante ML, Pirchi DE. Diagnostic yield of computed tomography guided fine-needle aspiration for pancreatic cancer. Medicina (B Aires). 2022; 82(5): 708-713. PMID: 36220027.
- Hsu MY, Pan KT, Chen CM, Lui KW, Chu SY, Lin YY, Hung CF, Huang YT, Tseng JH. CT-guided percutaneous core-needle biopsy of pancreatic masses: comparison of the standard mesenteric/retroperitoneal versus the trans-organ approaches. Clin Radiol. 2016; 71(6): 507-12. doi: 10.1016/j.crad.2016.02.021. Epub 2016 Mar 31. PMID: 27040800.
- Chaya C, Nealon WH, Bhutani MS. EUS or percutaneous CT/US-guided FNA for suspected pancreatic cancer: when tissue is the issue. GastrointestEndosc. 2006; 63(7): 976-8. doi: 10.1016/j.gie.2005.12.012. PMID: 16733112.
- Solass W, Struller F, Horvath P, Königsrainer A, Sipos B, Weinreich FJ. Morphology of the peritoneal cavity and pathophysiological consequences. Pleura Peritoneum. 2016; 1(4): 193-201. doi: 10.1515/pp-2016-0023. Epub 2017 Jan 10. PMID: 30911623; PMCID: PMC6328071.
- Gruber-Rouh T, Langenbach MC, Eichler K, Vogl TJ, Yel I, Beeres M. CT-guided percutaneous biopsy of suspect pancreatic lesions: radiological and clinical outcome. Clin Radiol. 2019; 74(11): 899. 7-899. 12. doi: 10.1016/j.crad.2021.03.004. PMID: 31495545.
- Sofocleous CT, Schubert J, Brown KT, Brody LA, Covey AM, Getrajdman GI. CT-guided transvenous or transcaval needle biopsy of pancreatic and peripancreatic lesions. J VascIntervRadiol. 2004; 15(10): 1099-104. doi: 10.1097/01.RVI.0000130815.79121.EC. PMID: 15466796.
- Lew SQ, Khan AA, Rieders B, Agrawal ST. Haemoperitoneum after an endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) of a pancreatic lesion in a peritoneal dialysis patient. BMJ Case Rep. 2020; 13(11): 236573. doi: 10.1136/bcr-2020-236573. PMID: 33148597; PMCID: PMC7643458.
- Hamada T, Yasunaga H, Nakai Y, Isayama H, Horiguchi H, Matsuda S, Fushimi K, Koike K. Severe bleeding and perforation are rare complications of endoscopic ultrasound-guided fine needle aspiration for pancreatic masses: an analysis of 3,090 patients from 212 hospitals. Gut Liver. 2014; 8(2): 215-8. doi: 10.5009/gnl.2014.8.2.215. Epub 2013 Nov 5. PMID: 24672664; PMCID: PMC3964273.
- Gupta S, Wallace MJ, Cardella JF, Kundu S, Miller DL, Rose SC; Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for percutaneous needle biopsy. J VascIntervRadiol. 2010; 21(7): 969-75. doi: 10.1016/j.jvir.2010.01.011. Epub 2010 Mar 20. PMID: 20304676.
- Brandt KR, Charboneau JW, Stephens DH, Welch TJ, Goellner JR. CT- and US-guided biopsy of the pancreas. Radiology. 1993; 187(1): 99-104. doi: 10.1148/radiology.187.1.8451443. PMID: 8451443.
- Amin Z, Theis B, Russell RC, House C, Novelli M, Lees WR. Diagnosing pancreatic cancer: the role of percutaneous biopsy and CT. Clin Radiol. 2006; 61(12): 996-1002. doi: 10.1016/j.crad.2006.07.005. PMID: 17097419.
- Tyng CJ, Almeida MF, Barbosa PN, Bitencourt AG, Berg JA, Maciel MS, Coimbra FJ, Schiavon LH, Begnami MD, Guimarães MD, Zurstrassen CE, Chojniak R. Computed tomography-guided percutaneous core needle biopsy in pancreatic tumor diagnosis. World J Gastroenterol. 2015; 21(12): 3579-86. doi: 10.3748/wjg. v21.i12.3579. PMID: 25834323; PMCID: PMC4375580.
- Smith EH. Complications of percutaneous abdominal fine-needle biopsy. Review. Radiology. 1991; 178(1): 253-8. doi: 10.1148/radiology.178.1.1984314. PMID: 1984314.
- Mueller PR, Miketic LM, Simeone JF, Silverman SG, Saini S, Wittenberg J, Hahn PF, Steiner E, Forman BH. Severe acute pancreatitis after percutaneous biopsy of the pancreas. AJR Am J Roentgenol. 1988; 151(3): 493-4. doi: 10.2214/ajr.151.3.493. PMID: 3261508.
- Ferrucci JT Jr, Wittenberg J, Mueller PR, Simeone JF, Harbin WP, Kirkpatrick RH, Taft PD. Diagnosis of abdominal malignancy by radiologic fine-needle aspiration biopsy. AJR Am J Roentgenol. 1980; 134(2): 323-30. doi: 10.2214/ajr.134.2.323. PMID: 6766240.
- Micames C, Jowell PS, White R, Paulson E, Nelson R, Morse M, Hurwitz H, Pappas T, Tyler D, McGrath K. Lower frequency of peritoneal carcinomatosis in patients with pancreatic cancer diagnosed by EUS-guided FNA vs. percutaneous FNA. GastrointestEndosc. 2003; 58(5): 690-5. doi: 10.1016/s0016-5107(03)02009-1. PMID: 14595302.