Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Nailing the chest pain
Akhil Munjal1,2*; Sudhir Prasada3
1Assistant Professor of Medicine, Campbell University School of Osteopathic Medicine, USA.
2Lead Hospitalist, Sound Physicians, UNC Health Nash, North Carolina, USA.
3Professor of Medicine, University of North Carolina School of Medicine, North Carolina, USA.
*Corresponding Author : Akhil Munjal
Assistant Professor of Medicine, Campbell University School of Osteopathic Medicine, USA.
Tel: 1-586-765-2526;
Email: dr.akhilmunjal@gmail.com
Received : Oct 29, 2024
Accepted : Nov 15, 2024
Published : Nov 22, 2024
Archived : www.jcimcr.org
Copyright : © Munjal A (2024).
Keywords: Angiography; Foreign body; Chest pain.
Citation: Munjal A, Prasada S. Nailing the chest pain. J Clin Images Med Case Rep. 2024; 5(11): 3354.
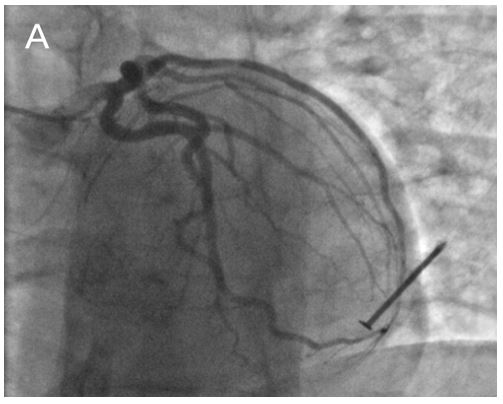
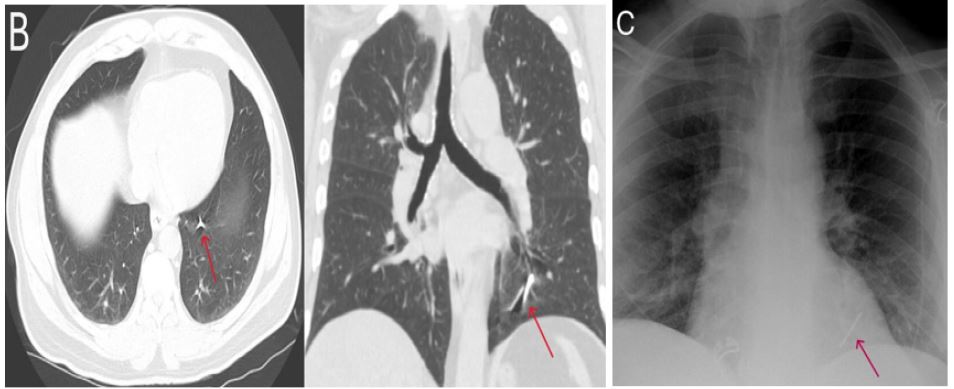
Description
A 64-year-old male with known HFrEF, hypertension and non-compaction cardiomyopathy presented for evaluation of chest pain and underwent an outpatient nuclear stress test. This showed a moderate to large, fixed, inferior apical defect and a stress LVEF of 17% which was similar to prior echocardiograms. Given concerning symptoms, a left heart catheterization was performed. On fluoroscopy, he was noted to have widely patent coronaries without any disease, however, he was surprisingly noted to have a metallic nail in the left hemithorax (Figure 1). Further imaging including a CT chest and chest x-ray localized the nail to be in the left lower lobe bronchus (Figure 2). A flexible bronchoscopy failed to locate the nail for retrieval due to its distal location. Eventually, he underwent a surgical wedge resection of the affected lobe for foreign body removal and has done well post procedurally. A screening chest x-ray for chest pain may have led to workup along a different and more appropriate route. The patient did not report any history of foreign body ingestion, further information from the patient’s wife revealed that he was in the habit of sleeping with a nail in his mouth and likely inhaled it in his sleep.