
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Colobomatous optic disc pit complicated by serous macular detachment: Report of two cases
Soda Mbaye*; Aïssatou Aw; El Hadji Malick Sy; Jean Pierre Diagne; Aly Mbara Ka; Mouhamed Ndiaye; Serigne Sohibou Gaye; Ousmane Ndiaga Senghor; Lamine Ndiaye; Papa Amadou Ndiaye
Abass Ndao University Hospital Center, Dakar, Senegal.
*Corresponding Author : Soda Mbaye
Abass Ndao University Hospital Center, Dakar, Senegal.
Email: soresm93@gmail.com
Received : Nov 25, 2024
Accepted : Dec 13, 2024
Published : Dec 20, 2024
Archived : www.jcimcr.org
Copyright : © Mbaye S (2024).
Abstract
Introduction: The discovery of Optic Disc Pit (ODP) during fundus examination is extremely rare. We report two cases of ODP complicated by maculopathy, diagnosed at the Ophthalmology Center of Abass Ndao Hospital, in order to highlight the specific characteristics of this condition.
Clinical observation: The first case involved a 37-year-old woman and the second a 31-year-old man, both of whom presented with unilateral Decreased Visual Acuity (DVA), evolving over 21 days for case 1 and 7 days for case 2, respectively. The visual acuity of the affected eye was 5/10 with correction in case 1 and counting fingers in case 2. Upon Fundus Examination (FE), an oval, grayish-white depression located temporally in case 1 and inferotemporally in case 2 was observed in the optic disc, corresponding to the Optic Disc Pit (ODP). In both cases, this was associated with a Serous Retinal Detachment (SRD) bubble. Optical Coherence Tomography (OCT) revealed schisis associated with SRD in both patients. Fluorescein Angiography (FA) showed hypo-fluorescence in the early phase and late hyperfluorescence in the area of the ODP. Therapeutic abstention was recommended for case 1, whilecase 2 was lost to follow-up.
Discussion: From a therapeutic standpoint, regular monitoring is indicated in asymptomatic cases to detect possible macular complications. The patient should be informed about the symptoms of macular complications and educated on self-monitoring. In cases of symptomatic maculopathy secondary to Optic Disc Pit (ODP-M), there is currently no consensus on management, and various therapeutic approaches have been attempted with variable success.
Conclusion: Our two cases highlight the importance of structured examination and monitoring of this condition. Moreover, when guiding management, it is essential to consider individual patient factors, as well as the risks and benefits of treatment.
Keywords: Maculopathy; Optic disc; Congenital; FA.
Citation: Mbaye S, Aïssatou A, El Hadji Malick S, Diagne JP, Aly Mbara K, et al. Colobomatous optic disc pit complicated by serous macular detachment: Report of two cases. J Clin Images Med Case Rep. 2024; 5(12): 3396.
Introduction
Optic Disc Pit (ODP) are associated with a dehiscence of the lamina cribrosa of the Optic Nerve (ON), causing a herniation of the dysplastic retina, which is bounded by a collagen wall. It is a rare congenital anomaly, occurring in 0.01 to 0.19% of the population. It appears sporadically and is unilateral in 85 to 90% of cases [1]. It is described as an atypical and incomplete coloboma of the ON head, usually located at the temporal margin, in contrast to a true coloboma, which generally affects the inferonasal region. Optic Disc Pit (ODP) is an isolated malformation that is usually asymptomatic and typically does not require any specific evaluation. However, it can be complicated by maculopathy in 25 to 75% of cases, known as maculopathy secondary to Optic Disc Pit (ODP-M), which involves foveoschisis and Serous Retinal Detachment (SRD), both leading to Decreased Visual Acuity (DVA) [2]. This ODP-M most often occurs in adults between the ages of 30 and 40, less frequently during adolescence, and rarely in young children [3]. It is often discovered during a routine Fundus Examination (FE) or in the presence of Decreased Visual Acuity (DVA). The diagnosis of maculopathy associated with Optic Disc Pit (ODP-M) has significantly benefited from the use of Optical Coherence Tomography (OCT), which highlights a characteristic feature: The presence of a connection between the optic nerve cavity and the intraretinal and/or subretinal space [4]. The therapeutic management of maculopathy secondary to Optic Disc Pit (ODP-M) is controversial. To date, no consensus exists, and various treatment strategies have been proposed, ranging from peripapillary photocoagulation to Light Amplification by Stimulated Emission of Radiation (LASER) and pars plana vitrectomy. The generally accepted approach is regular clinical follow-up with OCT, combined with self-monitoring for asymptomatic patients. In cases of Decreased Visual Acuity (DVA), vitrectomy surgery, potentially associated with other surgical procedures, appears to be the first-line recommended technique [5]. In Africa, there are few studies on Optic Disc Pit (ODP) and in our institution, this is the first work focused on this condition. With this in mind, we report two cases of Colobomatous optic disc pit complicated by serous macular detachment in order to elucidate the epidemiological, diagnostic, and therapeutic aspects of this condition.
Observations
Case 1
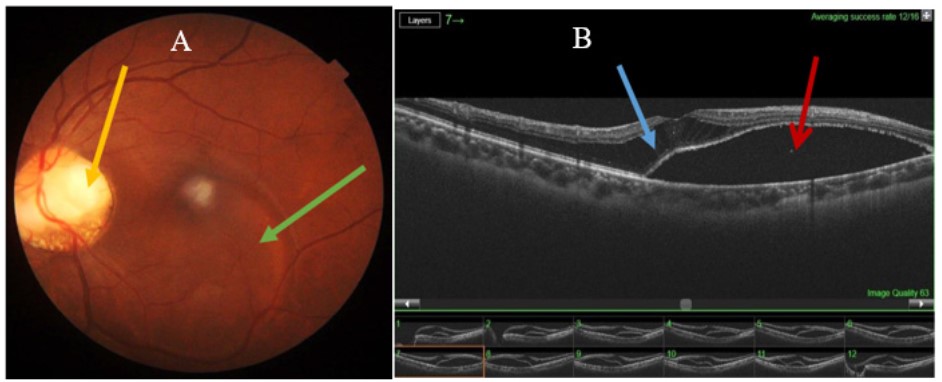
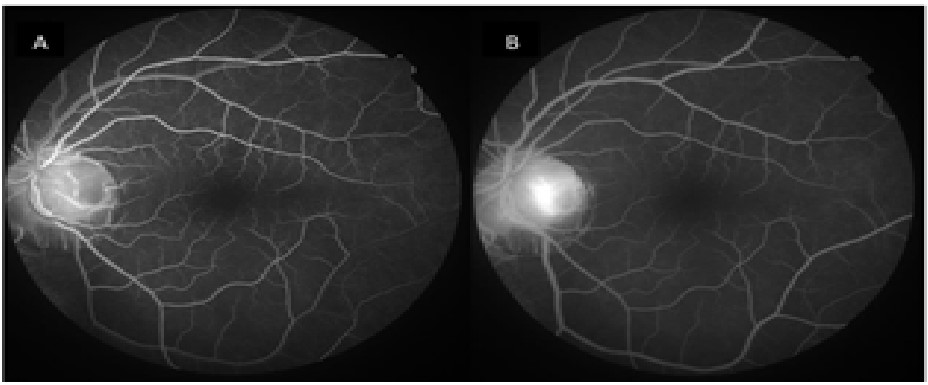
The patient was a 37-year-old woman with sickle cell disease(SS), who presented with rapidly progressive Decreased Visual Acuity (DVA) in the Right Eye (RE) evolving over the past three weeks. Upon ophthalmological examination, her uncorrected visual acuity was 2/10 in the RE and 9/10 in the Left Eye (LE). Corrected visual acuity was 5/10 in the RE and 9/10 in the LE. Anterior segment examination with a slit lamp revealed normal adnexa, anterior segment, and intraocular pressure in both eyes. Fundus Examination (FE) showed a large optic disc with an oval grayish-white depression located temporally, associated with a bubble of Serous Retinal Detachment (SRD) in the RE. A papillary coloboma was also noted inferiorly (Figure 1A). The fundus was normal in the LE. Optical Coherence Tomography (OCT) revealed serous macular detachment associated with schisis in the RE (Figure 1B). Fluorescein Angiography (FA) demonstrated early hypofluorescence of the Optic Disc Pit (ODP), which became hyperfluorescent in the late phase without leakage (Figure 2). Additionally, there were no signs of sickle cell retinopathy.
Given the corrected visual acuity of 5/10 in our patient, optical correction and regular monitoring were recommended.
Case 2
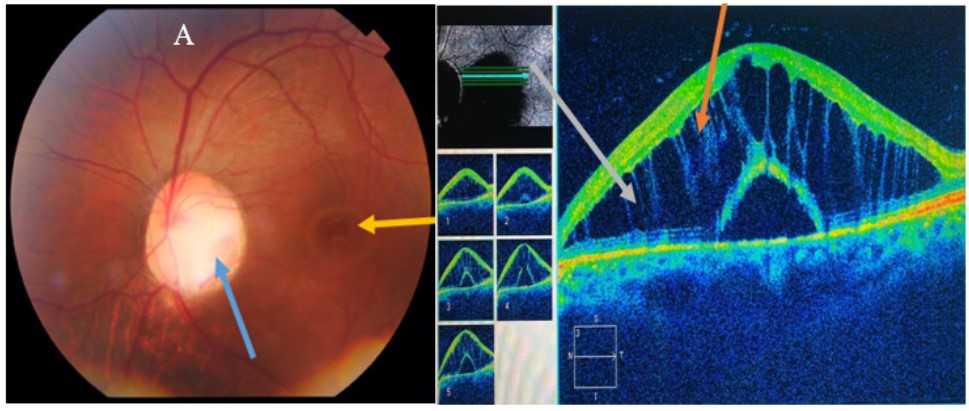
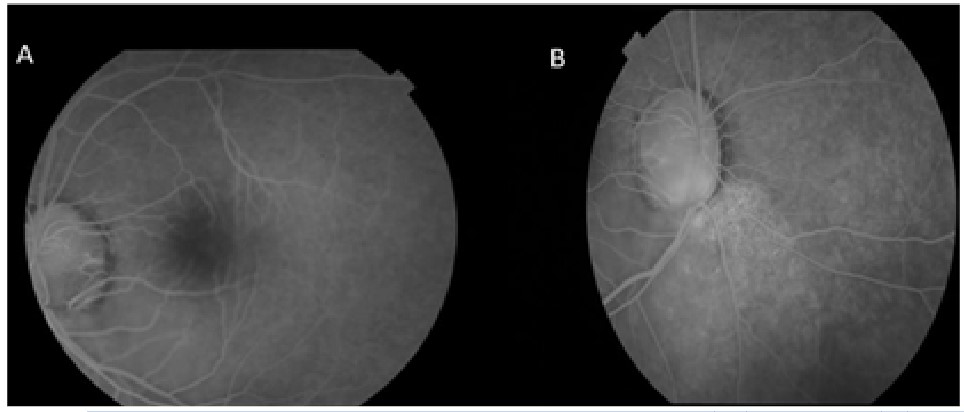
The patient was a 31-year-old man with no significant medical history, presenting with sudden onset of Decreased Visual Acuity (DVA) in the Left Eye (LE) that had been evolving for one week, with no history of trauma. Upon ophthalmological examination, uncorrected visual acuity was 10/10 in the Right Eye (RE) and “counting fingers at 5 meters” in the LE, not improved. Fundus Examination (FE) was normal in the RE, while in the LE, an oval grayish-white depression was noted inferotemporally in the optic disc, accompanied by a bubble of Serous Retinal Detachment (SRD) localized to the macular area (Figure 3A), along with inferopapillary chorioretinal atrophy and atypical vascular distribution at the optic disc. The OCT B-scan showed schisis associated with retrofoveolar SRD (Figure 3B). Fluorescein Angiography (FA) demonstrated the Optic Disc Pit (ODP) in the LE, which appeared initially hypofluorescent, then hyperfluorescent in the late phase, with an area of heterogeneous hyperfluorescence corresponding to the chorioretinal atrophy (Figure 4).
Discussion
Optic disc pit is a rare clinical entity that is part of the spectrum of congenital cavitary anomalies of the optic disc. It has been demonstrated to be an uncommon pathology, with a prevalence estimated between 0.01% and 0.19%. Its incidence is reported to be 2 per 10000. This low prevalence may also be related to the fact that it is a poorly understood condition, thus potentially underdiagnosed, especially in its uncomplicated form. In the literature, a diagnostic odyssey is frequently observed, with an initial diagnosis made in only 25% of cases. The majority of cases are sporadic, but autosomal transmission has been suggested in some families with multiple affected individuals. However, no specific genetic markers have been identified [1]. In our regions, there are few studies on Optic disc pit [2-4], in our institution, these are the first diagnosed cases.
Optic Disc Pit (ODP) is an asymptomatic condition in the absence of complications, which can be discovered at any age incidentally during a routine examination [6]. Maculopathy secondary to Optic Disc Pit (ODP-M), which is the primary circumstance of discovery, most often occurs in adults, less frequently during adolescence, and exceptionally in young children. In adults, it typically arises between the third and fourth decades of life, associated with changes in the vitreous [7]. Maculopathy secondary to Optic Disc Pit (ODP-M), which is the primary circumstance of discovery, most often occurs in adults, less frequently during adolescence, and exceptionally in young children. In adults, it typically arises between the third and fourth decades of life, associated with changes in the vitreous [8]. However, other authors note that maculopathy complicating ODP can occur at any age, particularly in older individuals, and may be confused with other conditions such as exudative Age-Related Macular Degeneration (AMD) [3,9].
No sex predominance has been reported [3,9]. ODP occurs equally in men and women and typically appears sporadically [10].
In cases of associated maculopathy, patients often complain of a recent and progressive decrease in Visual Acuity (VA) [9,11]. Depending on the degree of maculopathy, VA may range from 8/10 to “counting fingers.” According to some authors, a patient with maculopathy related to ODP generally has a VA of less than 3/10, and the onset time of Decreased Visual Acuity (DVA) is likely related to the speed of maculopathy development [12]. In our study, case 1 presented with rapidly progressive DVA with a VA of 5/10, while case 2 presented with sudden DVA with a VA of “counting fingers,” suggesting that the rapidity of maculopathy development could impact the severity of DVA. In a series of patients with maculopathy and ODP in Japan, central scotoma and metamorphopsia were the main reported signs [13].
The involvement was unilateral in both of our patients, as described in the majority of series [6,9]. Optic Disc Pit (ODP) can also be bilateral in 10 to 15% of cases [14]. In Marocco, Sayouti [15], reported a case of bilateral ODP in a young man complicated by maculopathy in one eye and uncomplicated in the other eye.
Optic disc pit of the optic nerve head vary in size, shape, color, depth, and location. Generally, they appear on Fundus Examination (FE) as a round or oval pit near the edge of the optic disc, often located in the inferotemporal quadrant, with a long axis parallel to the disc margin [8,16]. However, it has been reported that approximately 10 to 20% may be located at the center of the disc [14]. A study conducted in India [17], reported a case of unilateral double ODP, with both pits located in opposing disc segments; these were associated with macular SRD and atrophy of the Retinal Pigment Epithelium (RPE). In our study, the ODP was oval in shape, located temporally in case 1 and inferotemporally in case 2. It is usually grayish-white in color. However, in a study on a series of ODP cases in Greece, the authors reported ODP cases with gray color (60%), white/yellow (30%), and black (10%) [18]. This color variation may be related to fluid infiltration. In our study, they appeared grayishwhite in both cases. The size of the ODP can vary from oneeighth to one-quarter of the optic disc, potentially associated with thin tissue, most likely of a fibrous-glial nature surrounding the cavity. Although the appearance of the central retinal vessels is often normal in the majority of cases, in some cases, a small vessel may extend into the depth of the ODP and disappear, only to reappear on the other side [19]. In our study, case 1 had an associated inferior papillary coloboma, while case 2 exhibited inferopapillary chorioretinal atrophy and atypical vascular orientation at the optic disc.
ODP-M occurs in 25 to 75% of cases. Although it is a well-recognized clinical entity, it has not been conclusively established whether the subretinal fluid originates from the vitreous cavity, the subarachnoid space, or a leak from the retinal vessels around the optic disc. There are no obvious or known triggering factors for the development of this maculopathy. It typically begins with schisis of the inner retina, often having little or no impact on visual function and requiring no treatment, particularly as spontaneous resolution is possible. Subsequently, a serous detachment of the Retinal Pigment Epithelium (RPE) may complicate the schisis; this can result in lasting impairment of visual function, constituting an indication for surgical intervention [20]. On FE, it appears as a variable-sized circumscribed bubble encompassing the temporal edge of the optic disc and sometimes the entire posterior pole, frequently associated with remodeling of the RPE indicating chronicity. This maculopathy is primarily confused with central serous chorioretinopathy. Therefore, it is particularly important to search for the presence of a optic disc pit when evaluating a case of SRD or intraretinal schisis. In our series, the SRD bubble was larger in case 1 and extended to the inferior temporal arcade. Case 1 had sickle cell disease (SS), and no association with ODP has been reported in the literature.
Optical Coherence Tomography (OCT) has become the primary diagnostic and monitoring tool for maculopathy secondary to Optic Disc Pit (ODP-M). The typical OCT sign is the presence of a communication between the optic nerve cavity and the intraretinal and/or subretinal space. In some cases, an intrapapillary cavity is visible, corresponding to a hyporeflective area within the optic disc [2]. The appearance of this maculopathy is characteristic on OCT, combining schisis and serous macular detachment (SRD). However, in some cases, schisis can occur in isolation without SRD, and patients are often asymptomatic or less symptomatic [8]. Other studies have also identified associated macular holes through OCT [21]. In our two cases, schisis was associated with SRD. The accumulation of fluid was more significant in case 1 than in case 2, where there was a focal SRD. OCT also contributed to supporting hypotheses regarding the origin of retinal fluid. In one series, 100% of the eyes had fluid in the outer nuclear layer, and 53% had subretinal fluid along with retinal schisis. Based on these findings, the authors suggested that this fluid might likely penetrate the outer layer of the retina and then move in two possible directions: to the subretinal space and/or the inner layers of the retina [22]. OCT also plays a crucial role in cases of occult coloboma.
Fluorescein Angiography (FA) is generally unremarkable in cases of Optic Disc Pit (ODP). According to some authors, early hypofluorescence occurs, followed by late staining of the ODP without dye extension toward the macula or leakage from the pit. In other series, a defined area of late hyperfluorescence representing the area of macular elevation, without visible leakage points, has been reported [19]. In our two patients, the ODP appeared hypofluorescent in the early phase and hyperfluorescent in the late phase, with the hyperfluorescence being more pronounced in case 1. However, there was no defined area of hyperfluorescence indicating the SRD bubble.
Optical Coherence Tomography Angiography (OCT-A) identifies differences in capillary perfusion density between eyes with ODP and contralateral normal eyes. In a study correlating capillary perfusion density with the presence of ODP, a significant reduction in flow in the peripapillary radial plexus responsible for perfusion of the optic nerve head was reported in certain areas [23]. OCT-A in our two patients was limited by segmentation defects that biased interpretation. All types of Visual Field (VF) defects can be observed in ODP, whether associated with maculopathy or not. When maculopathy is established, it can lead to a central scotoma or other anomalies in the central VF [19]. The VF assessment was not performed in our two patients.
Currently, there are no widely accepted guidelines regarding the best management technique for maculopathy secondary to Optic Disc Pit (ODP-M) [8]. Various treatment modalities have been attempted with variable success. A conservative treatment approach involving laser photocoagulation of the temporal margin of the optic disc was initially proposed to create a watertight chorioretinal scar between the Optic Disc Pit (ODP) and the subretinal space. This technique requires careful attention to avoid damaging the macular retinal layers. The outcomes are inconsistent, with rates of reattachment reported to range from 80% to less than 15%, depending on the authors [19]. Some small case series have demonstrated absorption of the fluid with retinal reattachment, while others report very low success rates, often associated with severe visual field defects and no improvement in visual acuity [2,19]. Intravitreal gas injection with photocoagulation and positioning has subsequently been proposed as a therapeutic alternative to “pneumatically” displace the subretinal fluid away from the macula and improve visual acuity [2]. The technique involves performing two rows of 250-micron monochromatic laser spots on the temporal margin of the optic disc before or after injecting a bubble of 0.4 ml of pure Octafluoropropane (C3F8) into the vitreous. This injection, combined with anterior chamber paracentesis, is followed by positioning the patient face down for several hours a day for two to three weeks [24]. This technique has been employed in small case series and has resulted in visual improvement, although retinal reattachment occurred in only half of the cases [2,19]. However, the high recurrence rate, the occurrence of retinal detachment due to peripheral tears, and the role of vitreous traction in the development of maculopathy secondary to Optic Disc Pit (ODP-M) have led to the combination of this technique with vitrectomy. Vitrectomy, accompanied by posterior vitreous detachment, has become the first-line treatment. Internal limiting membrane peeling helps reduce and prevent macular retinal retractions but may lead to macular hole formation in some patients. For this reason, it is not systematically performed and is discouraged in cases of visible foveal thinning observed on fundus examination and optical coherence tomography (OCT) [24]. The benefit of peripapillary laser varies among authors. Some always combine it because it accelerates subretinal fluid reabsorption by stimulating retinal pigment epithelium cells. The rate of complete retinal reattachment after one year varies from 75% to 90%, with functional improvement in over 70% of patients [2,24]. Vitrectomy, the use of silicone oil for long-term tamponade is generally avoided, as there has been a reported case of intracranial migration through the ODP [25]. Another proposed approach is macular scleral buckling, which involves placing a scleral sponge at the posterior pole to limit intraretinal fluid migration and reduce vitreous traction on the juxta-papillary retina [2]. The anatomical and visual outcomes are excellent, with a complete resolution of fluid in approximately 85% of cases, associated with a significant improvement in Visual Acuity (VA). Long-term follow-up of these patients has shown that success was maintained for over 10 years, with very low rates of complications or recurrences [26]. However, it is important to note that despite these positive outcomes, the complexity of the surgical technique limits its widespread use. Additionally, several case series suggest covering the Optic Disc Pit (ODP) during surgery to prevent the passage of fluid into the intra- and subretinal spaces. The first description involved a case successfully treated with an injection of plateletrich plasma into the ODP. Other techniques include the use of an autologous scleral flap, the inverted Internal Limiting Membrane (ILM) flap technique over the ODP, or even the placement of a silicone punctal plug into the ODP [2,19]. In our study, we opted for conservative management with close monitoring in case 1 due to relatively preserved visual acuity at 5/10. For case 2, vitrectomy with Posterior Vitreous Detachment (PVD) induction and gas tamponade was considered.
According to Berrod [24], the progression of serous macular detachment is rarely favorable in the absence of surgical intervention. Once diagnosed, if Visual Acuity (VA) is preserved or greater than 5/10 on the Parinaud 4 scale, it may be acceptable to monitor the patient with an OCT performed every three to six months. In the absence of spontaneous resolution six months after the onset of maculopathy, surgical intervention is always recommended, as the chances of satisfactory functional recovery decrease beyond this time frame. The resorption of subretinal fluid is slow and may take several months. According to Sobol [27], the natural course of maculopathies associated with Optic Disc Pit (ODP) is often poor in the case of a Serous Retinal Detachment (SRD), as among 15 patients with pit-related maculopathy with SRD followed for 9 years, the final VA was less than 1/10 in 80% of cases. It was noted that in patients with isolated retinoschisis without SRD, after a mean follow-up of 40 months, only 14% required surgery, and VA was preserved over the follow-up period. Therefore, the mere presence of retinoschisis without SRD often has a limited impact on visual acuity. Patients presenting with retrofoveal SRD experienced spontaneous improvement in 19% of cases, with complete resolution of the SRD, and 50% of them required surgery. Among the patients who underwent surgery, there was no difference in visual and anatomical outcomes between those who had immediate surgery and those who had delayed surgery beyond six months. According to Sadun and Khaderi [28], in the medium and long term, cystic retinal degeneration, macular hole formation, or Retinal Pigment Epithelium (RPE) atrophy can occur. In our study, with a follow-up of 36 months, case 1 remains stable with preserved VA, while case 2 was lost to follow-up.
Conclusion
The Optic Disc Pit (ODP) is a rare clinical entity. It is estimated that it can complicate in 25 to 75% of cases with a maculopathy that involves schisis and/or serous retinal detachment. The pathophysiology of this maculopathy remains unclear. In our regions, there are few studies on ODP, making it difficult to determine its incidence. The literature, ODP is described as a sporadic and unilateral condition in 85 to 90% of cases, with no gender predominance. In the absence of complications, it is asymptomatic and often discovered incidentally. When maculopathy develops, the main symptom is reduced visual acuity, though other symptoms such as metamorphopsia and central scotoma have been reported. On fundus examination, the optic disc pit appears as a depression of varying shape, color, location, and size, sometimes associated with a Serous Retinal Detachment (SRD) bubble. Optical Coherence Tomography (OCT) has become an essential tool for diagnosing and monitoring this colobomatous maculopathy. Therapeutically, regular monitoring is recommended in asymptomatic cases to detect potential macular complications. The patient should be informed about the symptoms of macular complications and educated on selfmonitoring. In cases of Optic Disc Pit (ODP) complicated by maculopathy, there is currently no consensus on management, and various therapeutic modalities have been attempted with varying success. However, vitrectomy appears to be the firstline treatment to recommend. Additionally, individual patient factors, as well as the risks and benefits of the treatment, should be considered when planning the management approach.
Declarations
Conflict of interest: The authors declared that there were no conflicts of interest.
Funding: This research did not receive any specific grants from public, commercial, or non-profit funding bodies.
Ethical considerations: The collection of data from patient records was conducted in strict accordance with medical confidentiality.
References
- M M Uzel, M Karacorlu. Optic disk pits and optic disk pit maculopathy: A review. Surv. Ophthalmol. 2019; 64(5): 595-607. doi: 10.1016/j.survophthal.2019.02.006.
- G PH. Colobomatous optic disc pit a diagnosis not to be missed in cases of serous macular retinal detachment», Reality Ophtalmologic. Consulted on. 2024. https://www. realites-ophtalmologiques.com/2021/01/29/fossette-colobomateuse -un-diagnostic-a-ne-pas-manquer-en-cas-de-decollement-sereux-retinien-maculaire/.
- D Kalogeropoulos, et al. Optic Disc Pit Maculopathy - Case Series, Clinical Approach, and Management. Middle East Afr. J. Ophthalmol. 2020; 27(1): 34-9. doi: 10.4103/meajo.MEAJO_181_19.
- O Sandali, et al. Long-term results of the treatment of colobomatous optic disc pit complicated by serous macular retinal detachment: About 20 cases. J. Fr. Ophtalmol. 2011; 34(8): 532-38. doi: 10.1016/j.jfo.2011.03.010.
- Z Michalewska, Z Nawrocka, J Nawrocki. Swept-Source OCT and Swept-Source OCT Angiography before and after Vitrectomy with Stuffing of the Optic Pit. Ophthalmol. Retina. 2020; 4(9): 927-37. doi: 10.1016/j.oret.2020.03.025.
- I Chatziralli, G Theodossiadis, D Brouzas, P Theodossiadis. Incidence and Evolution of Subretinal Precipitates in Optic Disc Pit Maculopathy. Eur. J. Ophthalmol. 2017; 27(6): 769-73. doi: 10.5301/ejo.5000999.
- M C Bazard, L Stalnikiewicz, A Poirson, I Hubert, P Perriguey, et al. 548 optic disc pit and macular SDR. J. Fr. Ophtalmol. 2008; 31: 172. doi: 10.1016/S0181-5512(08)71146-X.
- E Rapizzi, P Gallon, D Ponzin, S Ferrari, N Zemella. A Conservative Surgical Approach to the Treatment of Optic Disc Pit Maculopathy: Four Case Reports. Case Rep. Ophthalmol. 2020; 11(2): 196-204. doi: 10.1159/000507880.
- G L Guern, A Couturier. Maculopathy associated with optic disk pit: monitoring and fllow-up. 2021.
- M Olszewski, M Marczak. Optic disc pit with maculopathy - a case report. Klin. Oczna. 2016; 118(4): 308-11.
- P Grassi, P Alexander. Spontaneous resolution of serous macular detachment and outer retinal defect in optic disc pit maculopathy », Clin. Exp. Optom. 2020; 3: 384‑385. doi: 10.1111/ cxo.12926.
- A Zheng, R P Singh, J A Lavine. Surgical Options and Outcomes in the Treatment of Optic Pit Maculopathy: A Meta-analysis and Systematic Review. Ophthalmol. Retina. 2020; 4(3): 289‑99, mars 2020, doi: 10.1016/j.oret.2019.10.011.
- F Bottoni, M Cereda, R Secondi, S Bochicchio, G Staurenghi. Vitrectomy for optic disc pit maculopathy: a long-term follow-up study. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2018; 256(4): 675-82. doi: 10.1007/ s00417-018-3925-9.
- A J Mangum. Case Report: Bilateral Cecocentral Visual Field Defect Secondary to Congenital Optic Disc Pit. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2022; 99(3): 308‑314. doi: 10.1097/ OPX.0000000000001864.
- A Sayouti, et al. 659 Bilateral colobomatous optic disk», J. Fr. Ophtalmol. 2008; 31: 200. doi: 10.1016/S0181-5512(08)71258- 0.
- N Panou, D G Vavvas. Optic Disk Pit with Sudden Central Visual Field Scotoma. Case Rep. Ophthalmol. Med. 2016; 2016: 1423481. doi: 10.1155/2016/1423481.
- N Babu, G Baliga, P Kohli, K Ramasamy. Management of double optic disc pit complicated by maculopathy », Indian J. Ophthalmol. 2020; 68(4): 663. doi: 10.4103/ijo.IJO_1114_19.
- I Georgalas, I Ladas, G Georgopoulos, P Petrou. Optic disc pit: A review Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2011; 249(8): 1113-22, août 2011, doi: 10.1007/s00417-011-1698-5.
- D Kalogeropoulos, et al. Optic Disc Pit Maculopathy: A Review. Asia-Pac. J. Ophthalmol. Phila. Pa. 2019; 8(3): 247-55. doi: 10.22608/APO.2018473.
- D Denis, et al. Congenital abnormalities of the disc. J. Fr. Ophtalmol. 2019; 42(7): 778-89. doi: 10.1016/j.jfo.2018.09.011.
- L Meng, X Zhao, W Zhang, D Wang, Y Chen. The characteristics of optic disc pit maculopathy and the efficacy of vitrectomy: A systematic review and meta-analysis. Acta Ophthalmol. (Copenh.). 2021; 99(7): e1176-e1189. doi: 10.1111/aos.14730.
- A Oli, D Balakrishnan. Treatment outcomes of optic disc pit maculopathy over two decades. Ther. Adv. Ophthalmol. 2021; 13: 25158414211027715. doi: 10.1177/25158414211027715.
- S Jiang, B Turco, N Choudhry. Vascular perfusion density mapping using optical coherence tomography angiography comparing normal and optic disk pit eyes. Retin. Cases Brief Rep. 2022; 16(1): 126‑132. doi: 10.1097/ICB.0000000000000908.
- JP Berrod. Management of Retinal Detachment Associated with optic disc pit. 2012.
- F Kuhn, F Kover, I Szabo, V Mester. Intracranial migration of silicone oil from an eye with optic pit. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2006; 244(10): 1360-1362. doi: 10.1007/s00417-006-0267-9.
- G P Theodossiadis, I P Chatziralli, P G Theodossiadis. Macular Buckling in Optic Disc Pit Maculopathy in Association with the Origin of Macular Elevation: 13-Year Mean Postoperative Results. Eur. J. Ophthalmol. 2015; 25(3): 241-248. doi: 10.5301/ ejo.5000553.
- W M Sobol, C F Blodi, J C Folk, T A Weingeist. Long-term Visual Outcome in Patients with Optic Nerve Pit and Serous Retinal Detachment of the Macula. Ophthalmology. 1990; 97(11): 1539-1542. doi: 10.1016/S0161-6420(90)32380-1.
- A A Sadun, K R Khaderi. Chapter 93 - Optic Disc Anomalies, Pits, and Associated Serous Macular Detachment, in Retina (Fifth Edition), S J Ryan, S R Sadda, D R Hinton, A P Schachat, S R Sadda, et al. Schachat, Éd. London: W.B. Saunders, 2013; 1583‑1588. doi: 10.1016/B978-1-4557-0737-9.00093-X.