
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Conservative management of pneumatosis intestinalis with spontaneous pneumoperitoneum: A compelling case report
Xia Zhao1; Jianguo Wang1; Ping Li1; Meng Wang2; Ning Wang3*
1Department of Radiology, Shandong University of Traditional Chinese Medicine Affiliated Hospital, Jinan 250014, China.
2Department of Gastrointestinal and Hernia Surgery, Shandong University of Traditional Chinese Medicine Affiliated Hospital, Jinan 250014, China.
3Department of Radiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan 250021, China.
*Corresponding Author : Ning Wang
Department of Radiology, Shandong Provincial
Hospital Affiliated to Shandong First Medical
University, Jinan 250021, China.
Email: 327242909@qq.com
Received : Dec 07, 2024
Accepted : Dec 26, 2024
Published : Jan 02, 2025
Archived : www.jcimcr.org
Copyright : © Wang N (2025).
Abstract
Background: Pneumatosis Intestinalis (PI) is a rare and often underrecognized medical condition, posing challenges for healthcare professionals. Accurate diagnosis is crucial to prevent unnecessary abdominal surgeries.
Case presentation: An 88-year-old patient with right thoracoabdominal pain was admitted to the Department of Thoracic Surgery. A post-admission Computed Tomography (CT) scan revealed PI extending from the distal ileum to the hepatic flexure of the colon. Conservative management, involving gas absorption, symptom resolution, and a return to normal dietary intake, was successfully employed.
Conclusion: Distinctive CT findings of PI are conducive to assessing the degree and extent of the condition. These observations provide robust evidence supporting both diagnosis and prognosis. Notably, our case challenges the current lack of consensus on treatment, suggesting that conservative treatment can be an effective alternative to surgicily intervention.
Keywords: Pneumatosis intestinalis; Computed tomography; Lung window setting; Case report.
Citation: Zhao X, Wang J, Li P, Wang M, Wang N. Conservative management of pneumatosis intestinalis with spontaneous pneumoperitoneum: A compelling case report. J Clin Images Med Case Rep. 2025; 6(1): 3408.
Introduction
Pneumatosis Intestinalis (PI) is characterized by the accumulation of gas within the intestinal wall. It is a complex process influenced by various factors, including genetic predispositions, bowel ischemia, inflammatory bowel diseases, systemic autoimmune diseases, organ transplantation, iatrogenic consequences (e.g., post-endoscopy/ colonoscopy or post-surgery), and certain pharmacological interventions (e.g., corticosteroids and chemotherapeutic agents). About 50% of cases of PI spontaneously resolve. Its incidence is unknown, mainly because most patients show no symptoms. Advances in CT scanning have increased the detection of asymptomatic cases. However, lack of medical understanding of this condition has led to misdiagnoses as digestive tract operations, resulting in unnecessary major surgeries [1]. At present, the optimal treatment approach for PI remains a topic of ongoing debate, with surgery not emerging as the primary intervention for asymptomatic patients [2]. Conservative treatment may serve as a viable option for patients with stable PI. This treatment involves parenteral nutrition, gastrointestinal decompression, fluid and electrolyte supplementation, antibiotics for bacterial infections, and oxygen or hyperbaric oxygen therapy. Treatment choices depend on a thorough assessment of the patient’s health, clinical presentation, medical history, and imaging results to determine the severity of PI. This report sheds light on a case involving a patient with PI extending from the distal ileum to the hepatic flexure of the colon, whose recovery was achieved through effective conservative management.
Case description
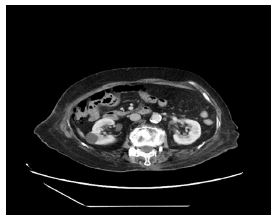
The Ethics Committee of the Shandong University of Traditional Chinese Medicine Affiliated Hospital waived the need for ethics approval because this study did not mention sensitive patient information and had no commercial interests. Written informed consent for publication was given by the patient. An 88-year-old woman, with a medical history encompassing hypertension, cardiac disease, interstitial pneumonia, rheumatoid and gouty arthritis, chronic hormone therapy, and a previous appendectomy for a low-grade mucinous tumor with calcification, presented to the Department of Thoracic Surgery at the Shandong University of Traditional Chinese Medicine Affiliated Hospital. Unfortunately, she was admitted to the ward due to worsening right thoracoabdominal pain persisting for 10 days. Upon admission, the patient complained of localized right thoracoabdominal pain, initially without fever, which later appeared in the afternoons, reaching a peak of approximately 38°C. A comprehensive laboratory evaluation showed an increase in leukocyte count (13.11×109/L), neutrophil count (9.68×109/L, 73.9% elevation), and monocyte count (1.56×109/L, 11.9% elevation), while a decline in lymphocyte count (1.8×109/L, 13.7%), ESR (14 mm/hr), and hypersensitivity C-reactive protein (CRP; 2.3 mg/L), and albumin (35.5 g/L) levels. Legionella pneumophila were found to be negative. The CT scan without contrast indicated the presence of extensive linear or bubbly gas within the intestinal wall, extending from the distal ileum to the hepatic flexure, and free air in the perirenal adipose tissue (Figures 1A, B). Specialized physical examination revealed a soft abdomen without gastrointestinal type or peristaltic waves, rebound pain, obvious abdominal muscle tension, or percussion or bowel sounds. Radiological assessments suggested a preliminary diagnosis of PI, without ruling out the possibility of a digestive tract perforation. Given the patient’s relatively benign clinical course without overt signs of an acute abdomen, a conservative management approach was adopted. This included gastrointestinal decompression, dietary restriction, venous nutritional support, mucosal protection, and anti-infection therapy. Fosfomycin sodium/cefoperazone sodium (6g/3g) plus omeprazole sodium (40 mg) were initiated once a day. Additionally, extracts from rabbit skin inflamed by vaccinia virus for injection ( ) were administered daily for pain relief. For nutritional support, fat emulsion amino acid (17%) glucose (11%) injection (1440 ml) and 50% glucose injection (200 ml) were administered daily. A subsequent 2-day follow-up CT displayed a substantial reduction in PI within the affected intestinal segment, a decrease in free gas within the perirenal space (Figure 1C). Laboratory findings demonstrated an increase in leukocyte count (9.68×109/L), neutrophil count (7.55×109/L, 78.1% elevation), and monocyte count (1×109/L, 10.3% elevation), while a decline in lymphocyte count (1.04×109/L, 10.7% reduction). After a 6-day treatment, a follow-up CT revealed near-complete absorption of gas in the in intestinal wall of the affected segment, along with full absorption of free gas in the perirenal space (Figure 1D). Laboratory results further confirmed an increase in leukocyte count (8.36×109/L), neutrophil count (5.97×109/L, 71.4% elevation), and monocyte count (0.96×109/L, 11.5% elevation), while a decline in lymphocyte count (1.23×109/L, 14.7% reduction). Furthermore, a Computed Tomography Angiography (CTA) imaging study uncovered mild proximal mesenteric artery stenosis, accompanied by atherosclerotic calcified plaque. Reduced blood flow to the intestines due to arterial stenosis and atherosclerosis can lead to tissue damage and compromise the integrity of the intestinal wall. This compromised integrity may allow gas to accumulate within the intestinal wall, leading to PI. Following conservative treatment, the patient experienced a gradual reduction in chest and back pain, and their body temperature returned to normal. The patient’s recovery progressed satisfactorily, allowing the resumption of a regular diet prior to discharge (Figure 2). Upon discharge, a structured regimen of periodic health check-ups is strongly recommended for the patient. If any discomfort or symptoms arise, seeking prompt medical attention is advised. In similar cases in clinical practice, timely CT scans should be conducted for accurate diagnosis. Although conservative treatment can be considered based on a thorough evaluation, it is crucial to closely monitor the patient and be prepared for potential emergency surgery.
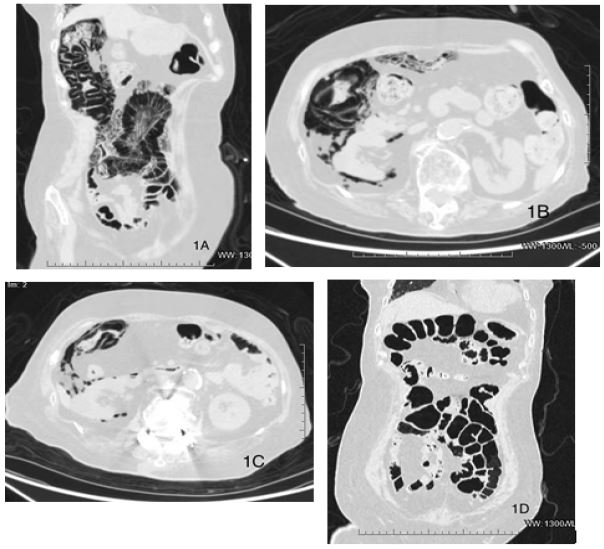
(C) Axial CT image through the lung window following 2 days of treatment. A discernible reduction in both the gas within the intestinal wall of the affected segment and the free gas localized in the perirenal space is observed.
(D) Coronal reconstruction CT image utilizing the lung window after 6 days of treatment. The gas previously identified in the intestinal wall of the diseased segment has been almost completely absorbed.
Discussion
PI, also known as pneumatosis cystoides intestinalis, manifests as the presence of gas within the intestinal wall, either observed during surgery or detected through radiological imaging. The condition is characterized by the accumulation of gas-filled cysts in the submucosal or subserosal layers of the gastrointestinal wall [1]. The pathogenesis of PI may involve intestinal diseases, systemic diseases, pulmonary conditions, medications, iatrogenic factors, and trauma. Although PI itself is not a disease, it serves as a clinical sign with a complex and multifactorial origin. Currently, there is no consensus on the treatment for PI, and surgery is not the initial choice for asymptomatic cases, as spontaneous resolution occurs in about 50% of instances [2]. Managing PI patients presents a complex challenge due to varied interpretations of its clinical significance and associated CT findings. This complexity adds a layer of difficulty for clinicians. The choice of treatment should stem from a thorough evaluation of the patient’s overall health, clinical presentation, medical history, and imaging results, discerning whether PI poses a benign or life-threatening risk. The general recommendation is to initially explore conservative medical and supportive treatments. For patients lacking the physical strength for surgery or anesthesia, surgical intervention is not advised. However, if CT confirms life-threatening symptoms such as intestinal perforation, obstruction, or portal vein gas accumulation, the likelihood of requiring surgical treatment significantly increases. Because the patient’s clinical course showed no apparent signs of acute abdomen, the decision was made to opt for conservative management. This approach involved gastrointestinal decompression, dietary restriction, venous nutritional support, mucosal protection, and anti-infection therapy. A daily regimen of fosfomycin sodium/cefoperazone sodium (6g/3g) plus omeprazole sodium (40 mg) was initiated. Additionally, once a day, injections of extracts from rabbit skin inflamed by vaccinia virus (3 ml) were administered for pain relief. Nutritional support included daily administration of fat emulsion amino acid (17%) glucose (11%) injection (1440 ml) and 50% glucose injection (200 ml).
Although there are many theories regarding the causes and development of PI, no single theory can explain all of the pathological processes. Basically, two primary theories contribute to the understanding of gas accumulation within the intestinal wall [3]. The bacterial theory proposes that gas pockets in PI originate from bacteria breaching the mucosal barrier, particularly during systemic infections. The mechanical theory posits that gas is propelled into the bowel wall due to direct injury or increased intraluminal pressure, which may occur in cases of pronounced luminal distension, intestinal obstruction, inflammatory bowel disease, ischemic bowel disease, gastroenteric tumors, or following certain interventions, such as colonoscopy, bowel preparation, anorectal surgery, or transplantation. During immune deficiency, the lymph nodes of the layer contract and the structural integrity is disrupted. Even if the pressure in the intestinal cavity is within the normal range, gas in the intestinal cavity can enter the intestinal wall and accumulate. Other theories, such as the pulmonary theory, nutritional deficiency theory, and chemical theory, offer additional perspectives on the potential origins of PI [4]. The pulmonary theory proposes that chronic obstructive pulmonary disease or cough causes alveolar rupture, with the gas spreading along the bronchial sheath to the mediastinum, abdominal cavity, mesentery, and intestinal wall. The nutritional deficiency theory proposes that long-term malnutrition leads to bacterial decomposition of nutrients in the intestine, thus producing gas that accumulates under the mucosa. The chemical theory proposes that long-term exposure to certain chemical substances or drugs can lead to the development of PI. PI manifests in two distinct forms: primary (idiopathic) and benign, which accounts for approximately 15% of cases, while secondary PI constitutes the remaining 85% [5]. Secondary PI has been associated with various disorders [6], such as bowel ischemia (53.7%), inflammatory bowel diseases (12.1%) [7], necrotic gastrointestinal diseases (8.1%), transmural ischemia or necrosis of the gastrointestinal wall [8], obstructive pulmonary disease, asthma, systemic autoimmune diseases, organ transplantation, barotrauma (e.g., during ventilation), iatrogenic consequences (e.g., post-endoscopy/colonoscopy or post-surgery), and certain pharmacological interventions (e.g., corticosteroids and chemotherapeutic agents) [9]. The clinical manifestations of PI span a wide spectrum, ranging from benign to potentially life-threatening forms [10]. While some patients may exhibit no symptoms, others may experience severe manifestations [11]. Common symptoms include abdominal pain, bloating, diarrhea, bloody stools and fever. In instances where giant gas cysts obstruct the intestinal cavity, complications such as intestinal obstruction, intussusception, or volvulus may arise. Rupture of gas cysts can lead to bloody stools, while the rupture or perforation of serosal cysts may result in pneumoperitoneum [1,3]. A review of the literature supports that PI, which typically affects the cecum and right colon, does not always indicate imminent bowel necrosis. Frequent symptoms include abdominal pain (54.5%) and distention (50%), accompanied by diarrhea, bloody stool, nausea, vomiting, and fever. Laboratory examinations and pathological biopsies of PI lack specificity, necessitating reliance on diagnostic modalities such as colonoscopy and imaging techniques, including CT, X-ray, and ultrasound. Abdominal upright films often reveal multiple small airbags in the projection area of the intestinal wall. CT, with its higher spatial resolution for anatomical structures, particularly when combined with lung window technology, is especially adept at displaying gas and offering crucial diagnostic information about the extent and severity of PI. Common radiological findings include pneumatosis within the intestinal wall, free air beneath the diaphragm, the identification of perforations, and the presence of gas in venous structures [12]. PI, characterized by the intraoperative or radiological identification of gas within the bowel wall, is diagnosed through imaging modalities such as X-ray, CT, and endoscopy, with CT recognized as the most sensitive and non-invasive diagnostic tool. Incidental detection of PI in CT scans often reveals multiple gas-filled cysts within the mucosa and submucosa of the small and/or large bowel [13]. The gastrointestinal wall is most frequently affected the ascending colon (55.2%) and the ileum (34.5%) [14]. In rare instances, the rupture of subserosal cysts of PI may lead to pneumoperitoneum without clinical peritonitis (< 3%) [15]. Diagnosing PI can pose challenges, particularly when gas is confined within the intestinal lumen, nestled between mucosal folds, or intermixed with feces. This resemblance to PI is especially pronounced when the gas is localized at a fixed site within the intestinal loop. When suspicion of PI arises, comprehensive evaluation through CT scans becomes imperative, employing both lung window and soft tissue window techniques for a thorough assessment, with continuous multilevel observation. Axial CT images prove most effective for diagnosing PI, offering insight into the gravity of the gas and aiding in determining its location, regardless of the intestinal lumen, the intestinal wall, or outside the intestinal wall. For enhanced visualization of the distribution and extent of gas within the intestinal wall, techniques such as thin-layer reconstruction, coronal reconstruction, and other multi-plane reconstruction methods can be employed. It is noteworthy that portal venous gas, which is an indicator of mesenteric ischemia, can also be observed in PI [16]. PI has a complication incidence of 16.3%, primarily attributed to intestinal obstruction (51.3%) or intestinal perforation (35.9%). Imaging findings indicative of clinically concerning PI encompass pneumatosis, free peritoneal fluid, and soft-tissue bowel wall thickening. On the contrary, the distribution, presence of free peritoneal air, and the characteristic morphology (linear vs cystic) of the gas do not necessarily signify an unfavorable prognosis [17]. As reported by Marc-Olivier Treyaud [18], the singular CT feature that significantly correlates with ischemia is the diminished contrast enhancement of the intestinal wall. In the specific instance of PI discussed in this paper, distinctive CT features were identified, suggesting a diffuse distribution of gas within the intestinal wall affecting the distal ileum and various regions of the colon (ascending colon and colon liver region). Moreover, the presence of free gas in the right perirenal space indicated the potential occurrence of spontaneous pneumoperitoneum, possibly stemming from air leakage following the rupture of an air cyst within the intestinal wall. Subsequent to this observation, two follow-up CT scans were executed: an unenhanced CT post a 2-day treatment and an enhanced CT after a 6-day treatment. The salient markers denoting improvement in the subsequent CT scans encompassed the reduction or absorption of gas within the intestinal wall and the abdominal cavity. Vigilant monitoring during follow-up CT scans was imperative to identify indications such as intestinal dilation, thickening of the intestinal wall, mesenteric fat edema and exudation, and the presence of gas in blood vessels. Notably, the physical examination and imaging assessment disclosed no signs of abdominal emergency or gas accumulation in the portal vein. The absence of abdominal free peritoneal fluid, soft-tissue bowel wall thickening, or portal vein gas further affirmed the benign nature of the case. Giant gas cysts have the potential to internally or externally compress the bowel lumen, resulting in the blockage of the intestinal cavity and, subsequently, leading to complications such as intestinal obstruction, intussusception, or volvulus. The rupture of gas cysts may, at times, lead to bloody stools, and the rupture or perforation of serosal cysts can result in pneumoperitoneum, a life-threatening condition [1,3]. Throughout the treatment course, the physician vigilantly monitored the patient using CT imaging, revealing a gradual absorption of gas in the affected intestinal wall. There were no complications such as portal vein gas accumulation or obstruction, and the patient’s symptoms showed improvement, substantiating the effectiveness of conservative treatment and the avoidance of surgery. The abdominal enhanced CT scan conducted in this study did not exhibit any reduction in the contrast enhancement of the intestinal wall. This occurrence could be attributed to the examination being conducted after the patient’s symptoms had ameliorated, and the majority of the gas had been absorbed. It is crucial to recognize that PI does not consistently signify acute abdominal symptoms such as gastrointestinal perforation. Determining the optimal management approach for PI patients poses a complex challenge due to different interpretations of the clinical significance of PI and its associated CT findings. Consequently, clinicians face a potentially intricate task in navigating the absence of a universally agreed-upon management strategy. However, it is noteworthy that surgery is not the initial preference for asymptomatic cases, as spontaneous regression occurs in approximately 50% of conservatively managed PI patients [2]. Treatment strategies vary widely, with specific methods for conservative care tailored to each patient’s unique circumstances. For instance, in cases of elevated white blood cell counts, assessing changes in lymphocytes, monocytes, and neutrophils can guide the selection of suitable antibiotics. If patients report abdominal pain, opting for intravenous nutrition instead of gastrointestinal nutrition may be a preventive measure against intestinal perforation or obstruction. In situations where symptoms persist or worsen, prompt imaging evaluations are essential, and preparations for emergency surgery should be initiated. Conservative treatments encompass a range of interventions such as parenteral nutrition, gastrointestinal decompression, fluid and electrolyte supplementation, antibiotic treatment for intestinal bacterial infections, and the application of oxygen or hyperbaric oxygen therapy. For the specific PI case examined in this study, a conservative therapeutic approach was pursued, involving gastrointestinal decompression, dietary restriction, venous nutritional support, mucosal protection, and anti-infection therapy. This course of action was dictated by the patient’s clinically benign trajectory, devoid of discernible indications of acute abdominal manifestations. Conservative treatment, characterized by its non-invasiveness, engenders a comparatively lesser psychological burden for patients and their families when dealing with the psychological complications associated with surgical interventions. This delineation renders conservative management a more psychologically amenable option for individuals undergoing treatment for PI. The selection of an appropriate treatment course hinges upon a thorough assessment of the patient’s overall health, clinical manifestation, medical background, and imaging results to ascertain whether the presence of PI poses a benign or life-threatening scenario. The prevailing recommendation leans towards initiating conservative medical and supportive measures as the initial approach. Ebrahimian M et al.’s study underscores the effectiveness of conservative treatment in the short term [19]. It is important to highlight that the efficacious implementation of conservative therapeutic measures not only obviated the necessity for surgical intervention but also substantially contributed to the enhancement of the patient’s overall health and recuperative trajectory. This substantial reduction in hospitalization duration not only translates into cost savings but also preserves invaluable temporal resources for the accompanying family. Additionally, the psychological well-being of both patients and their familial counterparts is expected to manifest a state of alleviated tension and improved positive affect. Nevertheless, surgical intervention becomes imperative when confronted with life-threatening complications, such as bowel obstruction, intussusception, massive hemorrhage, or the presence of portal vein gas. In cases where the PI patient maintains stability, the clinician may opt for an initial attempt at conservative treatment, closely monitoring the patient’s condition and conducting necessary imaging follow-ups as indicated [20]. The Endoscopic Fine-Needle Aspiration (EFNA) method emerges as a pragmatic alternative for PI treatment, circumventing the need for unwarranted surgical procedures [21]. In instances of sudden worsening symptoms, it is advisable to conduct a CT examination to eliminate the possibility of intestinal perforation, intestinal obstruction, or portal vein gas accumulation. Emergency surgery is highly probable under such circumstances. Patients afflicted with PI originating from gastrointestinal malignant tumors inevitably require surgical removal, highlighting the importance for clinicians to maintain vigilance for potential exacerbation of PI [22]. Whether opting for conservative or surgical intervention, a comprehensive evaluation of the individual patient’s overall health, clinical presentation, and medical history is imperative. The synergy of clinical and radiological imaging evaluations must guide the determination of whether the causative factor is benign or life-threatening, thereby informing the decision-making process for treatment strategies.
Conclusion
PI presents distinct CT manifestations that serve as valuable indicators for assessing the severity and extent of pneumatosis, along with secondary observations such as peritoneal free gas, ascites, portal gas, and malignant tumors. These manifestations not only contribute to the diagnostic process but also play a crucial role in evaluating prognosis. Conservative treatment options for PI involve implementing measures such as intestinal rest and antibiotic therapy. However, it is imperative to maintain close vigilance over the patient’s condition and conduct timely radiological follow-ups for monitoring PI progression. In cases where serious complications arise, surgical intervention may become necessary.
References
- Dhadlie S, Mehanna D, McCourtney J. Pneumatosis intestinalis a trap for the unwary: case series and literature review. International Journal of Surgery Case Reports. 2018; 53: 214-217. DOI: 10.1016/j.ijscr.2018.10.079.
- Aygüneş U, Karagün BŞ, Şaşmaz İ, et al. Pneumatosis cystoides intestinalis mimicking free intraabdominal air following chemotherapy for relapsed acute myeloblastic leukemia in a transplanted neutropenic child: a case report. TURKISH JOURNAL OF PEDIATRICS. 2023; 65(4): 693-697. DOI: 10.24953/turkjped.2023.116.
- Nureta TH, Moges TG, Abebe DM. Pneumatosis cystoides intestinalis associated with gastric outlet obstruction; A case report. International Journal of Surgery Case Reports. 2023; 111: 108828. DOI: 10.1016/j.ijscr.2023.108828.
- Ling F, Guo D, Zhu L. Pneumatosis cystoides intestinalis: a case report and literature review. BMC Gastroenterol. 2019; 19(1): 176. DOI: 10.1186/s12876-019-1087-9
- Gazzaniga G, Villa F, Tosi F, et al. Pneumatosis Intestinalis Induced by Anticancer Treatment: A Systematic Review. Cancers. 2022; 14(7): 1666. DOI: 10.3390/cancers14071666.
- Hwee Hong Lee A, Tellambura S. Pneumatosis intestinalis: Not always bowel ischemia. Radiology case reports. 2022; 17(4): 1305-1308. DOI: 10.1016/j.radcr.2022.01.062.
- Gao Y, Uffenheimer M, Ashamallah M, et al. Presentation and outcomes among inflammatory bowel disease patients with concurrent pneumatosis intestinalis: A case series and systematic review. Intest. Res. 2020;18: 289-296. DOI: 10.5217/ir.2019.00073.
- Sato T, Ohbe H, Fujita M, et al. Clinical characteristics and prediction of the asymptomatic phenotype of pneumatosis intestinalis in critically ill patients: A retrospective observational study. Acute Medicine & Surgery. 2020; 7: 556. DOI:10.1002/ams2.556.
- Wright NJ, Wiggins T, Stubbs BM, et al. Benign Pneumatosis intestinalis with pneumoperitoneum and Typhlitis: side-effects of drug or disease induced immunosuppression. BMJ Case Reports bcr. 2011; 0720114518.
- Kim SE, Lee SM, Kim JY. Blinatumomab-related pneumatosis intestinalis in a pediatric patient with relapsed acute lymphoblastic leukemia: A case report. J Oncol Pharm Pract. 2021; 27: 2045-2048.
- Alpuim Costa D; Modas Daniel P; Vieira Branco J. The Role of Hyperbaric Oxygen Therapy in Pneumatosis Cystoides Intestinalis A Scoping Review. Frontiers in Medicine. 2021; 8: 601872. DOI: 10.3389/fmed.2021.601872.
- Zhang T, Cao M, Zhao B, et al. Pneumatosis intestinalis post steroid use in a patient with immune-related adverse events: Case report, literature review and FAERS analysis. Frontiers in Pharmacology. 2023; 14: 1133551. DOI: 10.3389/fphar.2023.1133551.
- Ogul H, Pirimoglu B, Kisaoglu A, et al. Pneumatosis cystoides intestinalis: an unusual cause of intestinal ischemia and pneumoperitoneum. International Surgery. 2015; 100(2): 221-224.
- McKinley BJ, Santiago M, Pak C, et al. Pneumatosis Intestinalis Induced by Alpha-Glucosidase Inhibitors in Patients with Diabetes Mellitus. J. Clin. 2022; 11: 5918. DOI: 10.3390/jcm11195918.
- Ribolla M, Conti L, Baldini E, et al. Asymptomatic pneumoperitoneum in pneumatosis coli: a misleading operative indication. Int J Surg Case R. 2020; 69: 92-5. DOI: 10.1016/j.ijscr.2020.03.042.
- Wu LL, Yang YS, Dou Y, et al. A systematic analysis of pneumatosis cystoids intestinalis. World J Gastroenterol. 2013; 19: 4973-8. DOI: 10.3748/wjg.v19.i30.4973.
- Olson DE, Kim Y-W, Ying J, et al. CT predictors for differentiating benign and clinically worrisome Pneumatosis intestinalis in children beyond the neonatal period. Radiology. 2009; 253: 513-9. DOI: 10.1148/radiol.2532090168.
- Treyaud MO, Duran R, Zins M, et al. Clinical significance of pneumatosis intestinalis-correlation of MDCT-findings with treatment and outcome. Eur Radiol. 2017; 27(1): 70-79. DOI: 10.1007/s00330-016-4348-9.
- Ebrahimian M, Ghayebi N, Rezaee SP. Gastric pneumatosis and concurrent aeroportia due to gastric outlet obstruction: A case report. International journal of surgery case reports. 2021; 89: 106584. DOI: 10.1016/j.ijscr.2021.106584.
- Kielty J, Duggan W P, O’Dwyer M. Extensive pneumatosis intestinalis and portal venous gas mimicking mesenteric ischaemia in a patient with SARS-CoV-2. Annals of the Royal College of Surgeons of England. 2020; 102(6): 145-e147. DOI: 10.1308/rcsann.2020.0145.
- Takahashi K, Fujiya M, Ueno N, et al. Endoscopic Fine-Needle Aspiration Is Useful for the Treatment of Pneumatosis Cystoides Intestinalis with Intussusception. The American Journal of Gastroenterology. 2019; 114(1): 13. DOI: 10.14309/ajg.0000000000000069.
- Liu T, Zhang S, Mao H. Gastrointestinal malignant neoplasms disguised as pneumatosis cystoids intestinalis: A case report and literature review. Medicine. 2017; 96(51): 9410.