
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Primary cervical lymphoma to central nervous system invasion: A case report
Hongxiang An1; Jiacheng Yao2; Xuhong Zhang1*
1Radiotherapy Ward 2, Fushun Fourth Hospital, Fushun, Liaoning, China.
2Radiotherapy Department, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning, China.
*Corresponding Author : Xuong Zhang
Radiotherapy Ward 2, Fushun Fourth Hospital, Fushun, Liaoning, China.
Email: anx1985@163.com
Received : Dec 05, 2024
Accepted : Dec 26, 2024
Published : Jan 02, 2025
Archived : www.jcimcr.org
Copyright : © Xuhong Z (2025).
Abstract
69-year-old woman presented with a rare and sporadic case of diffuse large B-cell lymphoma of the primary cervix. Following pathological diagnosis, rituximab and chemotherapy combined with radiotherapy were administered. Nearly five years later, she developed an exceptionally rare central nervous system infection.
Keywords: Primary cervix; Diffuse large B cell lymphoma; Central nervous system invasion.
Citation: Hongxiang A, Jiacheng Y, Xuhong Z. Primary cervical lymphoma to central nervous system invasion: A case report. J Clin Images Med Case Rep. 2025; 6(1): 3409.
Case presentation
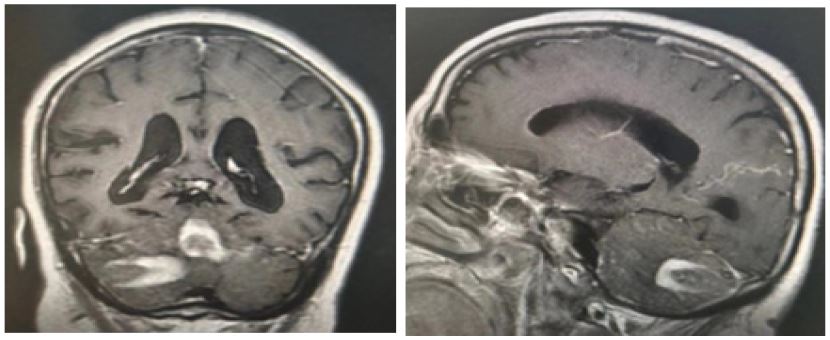
In March 2024, a 69-year-old woman presented with “a 5-year history of cervical lymphoma and a 3-month history of headache.” On April 29, the patient sought attention for persistent vaginal bleeding. Pelvic enhanced Magnetic Resonance Imaging (MRI) revealed a circular cervical mass measuring approximately 6.0 × 5.3 × 5.6 cm, continuous cervical mucosa compression, continuous thinning cervical stromal layer, continuous cervical outer membrane surface, and filling of the vaginal vault with mass signal. Imaging diagnosis indicated that cervical space mass was consistent with lymphoma changes (Figure 1). A gynecological examination revealed that the cervix had significantly increased, with a diameter of 5.5 cm. The cervix exhibited ulcerative necrosis, dark red congestion, and medium tissue quality. Immunohistochemistry of the biopsy tissue revealed CD10 (−), Ki-67 (70%), CD3 (−), CD20 (+), CD56 (−), BCL-6 (+), MUM 1 (−), and CD79 ɑ (+). The pathological diagnosis was Non-Hodgkin’s Lymphoma (NHL, diffuse large B-cell origin). Systemic enhanced Computed Tomography (CT) and superficial lymph nodes revealed no abnormalities, and no tumor cells were observed in the bone marrow biopsy. The diagnosis was cervical Diffuse Large B-Cell Lymphoma (DLBCL), classified as Ann Arbor Stage IE, with an international prognostic index of 1 and an ECOG score of 0. Before physical health, between April and July 2019, four cycles of R-CHOP chemotherapy were performed. Tumor lesions decreased in size after two cycles but increased by the fourth cycle. Owing to impaired cardiac and pulmonary function, a consultation was impossible. Using IMRT, cervical extracorporeal radiotherapy was administered at 50 Gy, 2 Gy, and 25 f between August and September 2019, and the cervical lesions disappeared (Figure 2). Two additional cycles of CHOP chemotherapy were performed between October and November 2019. Regular follow-ups revealed no abnormality. Three months earlier, the patient developed a headache accompanied by dizziness but no jet-like vomiting. Cranial MRI revealed bilateral abnormal signals in the cerebellar hemisphere and vermis with enhancement, suggestive of cerebellar and meningeal metastases (Figure 3). No abnormalities were observed in systemic enhanced CT and superficial lymph nodes. The patient refused invasive examination, including bone marrow puncture, lumbar puncture, and radiotherapy. The patient received two cycles of chemotherapy with “vindoisine + etoposide + prednisone,” which improved symptoms. The patient discontinued treatment after three cycles.
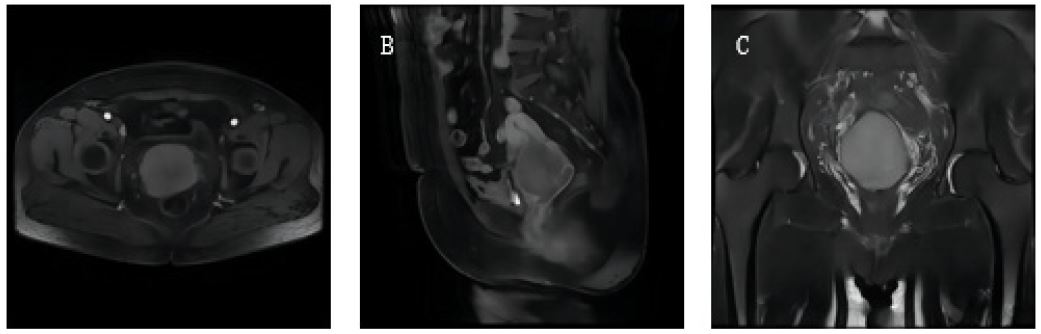
Note: A, B and C show axial, sagittal, and coronal images of cervical lesions respectively.
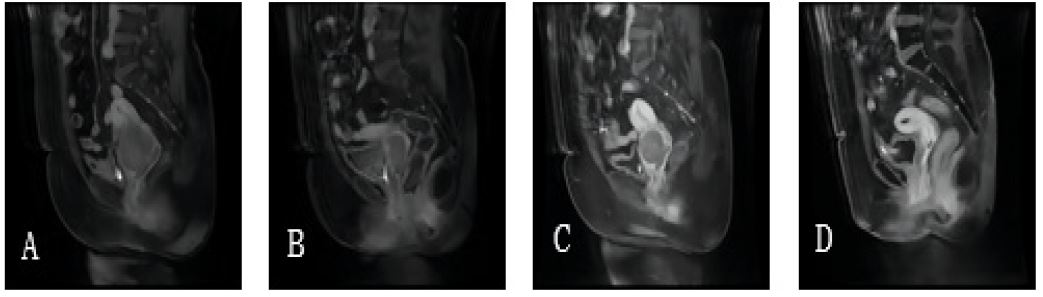
Note: A: Initial onset; B: 2 cycles of R-CHOP; C: 4 cycles of R-CHOP; D: 1 month after radiotherapy.
Discussion
Primary cervical lymphoma is extremely rare, and secondary Central Nervous System (CNS) invasion is rarely reported. DLBCL is an NHL originating from B lymphocytes, with a diffuse distribution of malignant large B lymphocytes in tumor tissue. DLBCL accounts for 33%-45% of all NHL, while extranodal primary lymphomas account for 35%-40% of all NHL. B cell-derived primary extranodal lymphomas are commonly found in the gastrointestinal tract, head, neck, and other sites, including the lungs, breast, uterine adnexa, testis, and CNS. The staging and treatment approaches for primary extranodal lymphoma are similar to those for patients with primary intranodal lymphoma. Primary Lymphoma of the Female Genital Tract (PLFGT) is rare, accounting for 0.5%-1.5% of all extranodal NHL and about 0.008% of gynecological tumors [1], it predominantly occurs in postmenopausal women, with a median age of onset of 54 years. The main pathological types are DLBCL and follicular lymphoma [2]. The ovaries and cervix are the frequently affected sites, most of which lack the B symptoms associated with lymphoma: Low fever, fatigue, night sweats, and weight loss. The most common symptom is vaginal bleeding [3-5]. For the cervical lymphoma staging, the Ann Arbor system and the International Union of Obstetrics and Gynecology (FIGO) system can be used. Treatment strategies are not well-established and rely mainly on case reports and small sample case series. Treatment options include surgery, chemotherapy, and radiotherapy alone or in combination [6,7]. Young patients can also be treated by preserving reproductive function [8]. Most cases are treated with the R-CHOP regimen [9]. Reports of spontaneous regression of the lymphoma are even rarer [10]. A retrospective study indicated an increased risk of CNS recurrence in primary female reproductive tract DLBCL [11,12]. More evidence is needed to support CNS prophylaxis. Risk factors for CNS invasion by DLBCL include the primary sites of the disease (testis, paranasal sinus, epidural, and bone marrow), HIV lymphomas, more than two extranodal sites, and elevated LDH levels [13]. Review of relevant literature for CNS infection secondary to PLFG. While there are no reports of the metastasis of the disease, direct invasion into the bladder may be considered. Symptoms of CNS invasion in lymphoma include confusion, headache, lethargy, and hemiparesis. The most common manifestations are leptomeningeal metastasis, epidural spinal cord compression, and brain parenchymal infiltration, which can be confirmed by cerebrospinal fluid analysis, brain CT/MRI, and sometimes, brain biopsy [11]. In this case, the patient did not present with either risk factor; however, imaging confirmed brain parenchymal infiltration and meningeal metastasis. There is no reasonable explanation for why secondary CNS involvement occurred. The therapeutic response to recurrent NHL, particularly in the CNS, has been unsatisfactory. Rapid control of CNS involvement is crucial to prevent neurological morbidity and preserve the quality of life. Close attention should be paid to the potential for CNS spread, and if neurological symptoms develop, prompt diagnostic evaluation, such as a brain MRI scan and lumbar puncture, should be conducted. Once patients are diagnosed with CNS infection, treatment should include radiotherapy, intrathecal injection of chemotherapy drugs, and systemic chemotherapy. This disease is rare, and high-quality research is lacking; therefore, there is no consensus on the best treatment approach yet.
Conclusion
Based on case reports and a review of available literature, primary cervical DLBCL is rare, and secondary CNS involvement is even rarer, as only mentioned in a retrospective study [11]; no detailed cases have been reported. Patients with such cases need individualized treatment. We presented a case of rare primary cervical DLBCL, where the chemotherapy response was poor. However, local radiotherapy enabled the patient to achieve disease-free survival for nearly 5 years. Later, secondary CNS invasion occurred, and systemic chemotherapy provided some survival benefits. Owing to the low incidence of primary cervical NHL, there is a lack of large-sample and long-term research reports, hence requiring further exploration of diagnosis, treatment standardization, and prognosis. Although secondary CNS invasion from cervical lymphoma exists, the specific metastasis pathway remains unclear. We recorded a case; thus, prospective studies are needed to determine the optimal treatment approach.
References
- Lagoo AS, Robboy SJ. Lymphoma of the Female Genital Tract: Current Status. International Journal of Gynecological Pathology. 2006; 25(1): 1-21. doi: 10.1097/01.pgp.0000183049.30212.f9.
- Weng X, Huang M, Zhang M, Yang Y, Liu X, et al. Primary lymphoma of the uterine cervix: A clinicopathologic study of 13 cases with review of additional 54 cases in the literature. Virchows Archiv. 2022; 482(2): 419-29. doi:10.1007/s00428-022-03436-y.
- Nasioudis D, Kampaktsis PN, Frey M, Witkin SS, Holcomb K. Primary lymphoma of the female genital tract: An analysis of 697 cases. Gynecologic Oncology. 2017; 145(2): 305-9. doi: 10.1016/j.ygyno.2017.02.043.
- Peng F, Li J, Mu S, Qin Y, Ma J, et al. Epidemiological features for primary lymphoma of the female genital tract patients and development of a nomogram to predict survival. Annals of Medicine. 2022; 54(1): 962-76. doi:10.1080/07853890.2022.2046289.
- Ensor AM, Sanchez CG, Ensor JE, Anand K. Primary diffuse large B-cell lymphoma of the uterus. Medicine. 2021; 100(40). doi:10.1097/md.0000000000027359.
- Stabile G, Sancin L, Boschian Bailo P, Ripepi C, Romano A, et al. Hysteroscopic Resection Followed by Adjuvant Radiotherapy: Report of a New Therapeutic Approach to Primary Cervical Diffuse Large B-Cell Lymphoma. International Journal of Environmental Research and Public Health. 2022; 19(18). doi:10.3390/ijerph191811779.
- Capsa C, Calustian LA, Antoniu SA, Bratucu E, Simion L, et al. Primary Non-Hodgkin Uterine Lymphoma of the Cervix: A Literature Review. Medicina. 2022; 58(1). doi:10.3390/medicina58010106.
- Stabile G, Ripepi C, Sancin L, Restaino S, Mangino FP, et al. Management of Primary Uterine Cervix B-Cell Lymphoma Stage IE and Fertility Sparing Outcome: A Systematic Review of the Literature. Cancers. 2023; 15(14). doi:10.3390/cancers15143679.
- Pfreundschuh M, Kuhnt E, Trümper L, Österborg A, Trneny M, et al. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. The Lancet Oncology. 2011; 12(11): 1013-22. doi:10.1016/s1470-2045(11)70235-2.
- Desana B, Balbo Mussetto A, Macera A, Mariani L, De Rosa G,et al. Rare case of uterine cervix lymphoma with spontaneous regression: Case report. Journal of Obstetrics and Gynaecology Research. 2020; 47(2): 807-11. doi:10.1111/jog.14562.
- Cao X-x, Li J, Zhang W, Duan M-h, Shen T, et al. Patients with primary diffuse large B-cell lymphoma of female genital tract have high risk of central nervous system relapse. Annals of Hematology. 2014; 93(6): 1001-5. doi:10.1007/s00277-013-2003-y.
- Yun J, Kim SJ, Won JH, Choi CW, Eom HS, et al. Clinical features and prognostic relevance of ovarian involvement in non-Hodgkin’s lymphoma: A Consortium for Improving Survival of Lymphoma (CISL) report. Leukemia Research. 2010; 34(9): 1175-9. doi: 10.1016/j.leukres.2010.02.010.
- Zelenetz AD, Wierda WG, Abramson JS, Advani RH, Andreadis CB, et al. Non-Hodgkin’s Lymphomas, Version 3.2012. Journal of the National Comprehensive Cancer Network. 2012; 10(12): 1487-98. doi:10.6004/jnccn.2012.0155.