
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Transfacial approach to an undifferentiated sinonasal carcinoma
Beatriz Ramada1*; Tiago Lopes1; Nuno Silva1; João Neves1; João Elói1,2; Jorge Miguéis1,2
1Otorhinolaryngology Department, Local Health Unit of Coimbra, Coimbra, Portugal.
2Otorhinolaryngology University Clinic, Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
*Corresponding Author : Beatriz Ramada
Otorhinolaryngology Department, Local Health Unit of Coimbra, Coimbra, Portugal.
Email: beatrizramada@gmail.com
ORCID: 0000-0001-9597-4024
Received : Dec 09, 2024
Accepted : Dec 27, 2024
Published : Jan 03, 2025
Archived : www.jcimcr.org
Copyright : © Ramada B (2025).
Abstract
Sinonasal undifferentiated carcinoma is a rare and aggressive tumour of the nasal cavity. Treatment involves a multimodal approach: surgical resection, radiotherapy and/or concurrent chemotherapy. A 58-year-old female presented with pain in the medial wall of the left orbital cavity, persisting for one month. Computed tomography revealed an expansive lesion centred in the left frontal sinus with bone erosion with extension into the anterior cranial cavity. Magnetic resonance imaging showed intracranial and infraorbital lesion expression, causing slight brain moulding, dural thickening/enhancement and deformation of the extrinsic ocular musculature. The biopsy confirmed sinonasal SMARCB1-deficient carcinoma (undifferentiated). Surgical tumour excision was carried out using a combined approach with the Neurosurgery Service. The tumour mass was removed in bloc. In the postoperative period, the patient underwent radiotherapy but experienced tumour recurrence culminating in death approximately four months after the initial diagnosis. This case highlights the high morbidity and mortality associated with undifferentiated sinonasal carcinomas, emphasizing the need for research into new treatment strategies.
Keywords: Sinonasal carcinoma; Transracial approach.
Citation: Ramada B, Lopes T, Silva N, Neves J, Elói J, et al. Transfacial approach to an undifferentiated sinonasal carcinoma. J Clin Images Med Case Rep. 2025; 6(1): 3411.
Introduction
Sinonasal Undifferentiated Carcinoma (SNUC) is a rare and aggressive tumour of the nasal cavity. Imaging has a good potential diagnostic value for SNUC [1], as it has been shown to have a lower Apparent Diffusion Coefficient (ADC) ratio than adenoid cystic carcinoma, but a higher Fluorodeoxyglucose (FDG) than esthesioneuroblastoma. These tumours arise most frequently in the nasal cavity and ethmoid sinuses, and most present as very large masses involving multiple sites [2,3]. According to the WHO, no consistent aetiology of SNUC has been identified [3]. Despite large primary tumour size, nodal metastases are uncommon but the majority spreads beyond the sinonasal tract to adjacent sites as the orbital apex, skull base and brain [4]. Since most patients are asymptomatic until advanced stages [1,2], it has a poor prognosis, with a mortality rate exceeding 70% [2]. In fact, around 80% of patients are diagnosed at the T4 stage [2].
Currently, the SMARCB1 (INI-1-)-deficient sinonasal carcinoma is not a distinct entity according to the WHO [3]. Clinical and histologic features are very similar to the SNUC, although some differences can be found. Imaging features as Fluorodeoxyglucose (FDG) avidity, hypo-or iso- intensity in T2 sequences and restriction are similar but calcifications are more commonly found in INI-1-deficient sinonasal carcinomas [2]. Since the loss of INI-1 conducts to a diminished transcription on cyclin D1, this protein is a potential therapeutic target in the future [4]. Treatment requires a multimodal approach: surgical resection (if feasible), radiotherapy, and/or concurrent chemotherapy [2].
Case presentation
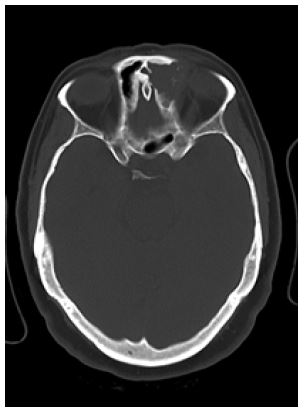
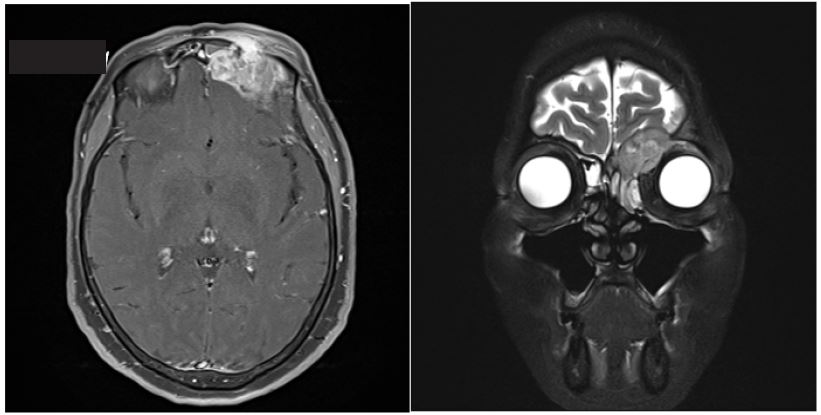
A 58-year-old female presented with pain in the medial wall of the left orbital cavity, persisting for one month. Computed Tomography (CT) revealed an expansive lesion centred in the left frontal sinus with bone erosion of its walls and extension into the anterior cranial cavity (Figure 1). Magnetic Resonance Imaging (MRI) showed intracranial and intraorbital lesion expression, causing slight brain moulding, dural thickening/enhancement, and deformation of the extrinsic ocular musculature (Figures 2 and 3).
A biopsy performed via endonasal endoscopic access confirmed sinonasal SMARCB1-deficient carcinoma.
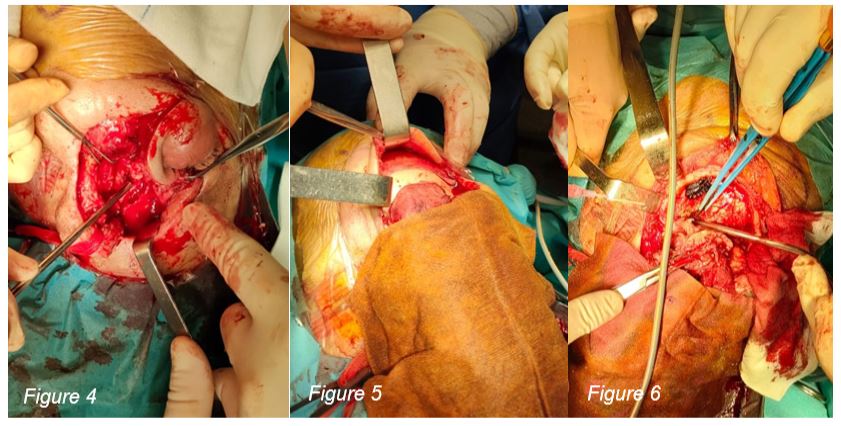
Surgical tumour excision was carried out using a combined approach with the Neurosurgery Service, starting with a lateral rhinotomy incision extended to the supraciliary region. This method allowed the creation of a naso-orbito-frontal flap, enabling partial maxillectomy, anterior and posterior ethmoidectomy, and fronto-orbital craniectomy. The tumour mass was removed en bloc, and the defect was closed with a pedicled epicranial aponeurosis flap and a titanium mesh for reconstruction of cranial vault, orbital rim and roof. The following images illustrate the procedure.
Conclusion
The lesion’s features and clinical presentation align with those described in the literature, namely its infiltrative nature, nasoethmoidal location with orbital and skull base extension and diagnosis typically occurring between the age of 50-60. The exception is the absence of calcifications on imaging studies. Sinonasal undifferentiated carcinoma is challenging to treat, and currently, there is no standard treatment protocol. This case highlights the high morbidity and mortality associated with these tumours, emphasizing the need for research into new treatment strategies.
Declarations
Authors contributions: BR: review the literature and wrote the draft of the manuscript. Followed the patient in the outpatient setting. TL, NS, JN, JE and JM: Critical review of the article.
Acknowledgements: The authors would like to acknowledge Dr. Armando Lopes, Neurosurgeon from ULS Coimbra.
Funding source: The authors do not receive a specific grant from any funding agency in the public, commercial or not-for- profit sectors.
Protection of humans and animals: The authors declare that the procedures were followed according to the regulation’s es tablished by the Clinical Research and Ethics Committee and to the Helsinki Declaration of the World Medical Association updated in 2013.
Competing interests: The authors declare that there is no competing interest.
Patient consent: Consent to publish the case report was obtained.
Data confidentiality: The authors declare having followed the protocols in use at their working center regarding patients’ data publication.
References
- Agaimy A, Hartmann A, Antonescu CR, Chiosea SI, et al. SMARCB1 (INI-1)-deficient sinonasal carcinoma: a series of 39 cases expanding the morphologic and clinicopathologic spectrum of a recently described entity. Am J Surg Pathol. 2017; 41(4): 458-471.
- Contrera KJ, Woody NM, Rahman M, Sindwani R, et al. Clinical management of emerging sinonasal malignancies. Head Neck. 2020; 42: 2202-2212.
- El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. WHO Classification of Head and Neck Tumours (4th Edition). IARC 2017. ISBN 978-92-832-2438-9.
- Anchaal K, Mariadas AV, Raja P, Pirabu S, Chirom Aset al. SMARCB1 (INI1)–deficient sinonasal carcinoma: a series of 13 cases with assessment of histologic patterns. Human Pathology. 2019; 83: 59-67.