
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Effective use of lymphangiography and embolization in chyle leak following neck surgery
Reut Book1*; Itamar Tamir2; Raphael Wolf1; Menachem Gross1,3
1Department of Otolaryngology - Head and Neck Surgery, Hadassah Medical Center, Jerusalem, Israel.
2Department of Radiology, Hadassah Medical Center, Jerusalem, Israel.
3Faculty of Medicine, Hebrew University, Jerusalem, Israel.
*Corresponding Author : Reut Book
Department of Otolaryngology - Head and Neck Surgery, Hadassah Medical Center, Jerusalem, Israel.
Tel: +972-2-6776469, Fax: +972-2-6435090;
Email: reutbook@Gmail.com
Received : Dec 09, 2024
Accepted : Dec 30, 2024
Published : Jan 06, 2025
Archived : www.jcimcr.org
Copyright : ©Book R (2025).
Abstract
Background: Chyle leaks are a rare but significant complication following neck surgery, particularly after thyroidectomy or lateral neck dissection. These leaks, if not promptly identified and treated, can lead to severe complications such as malnutrition, electrolyte imbalances, and immunosuppression.
Case presentation: A 33-year-old woman presented with progressive neck swelling six weeks after a total thyroidectomy and left neck dissection for papillary thyroid carcinoma. Initial imaging revealed a large fluid collection compressing the trachea and jugular vein, suggesting a chyle leak. Surgical drainage confirmed chyle leakage, and despite conservative management, the leak persisted. Lymphangiography identified the leak site, and successful embolization using histoacryl glue resolved the issue.
Conclusion: This case underscores the importance of flexible management of chyle leaks. While conservative treatments are effective for low-output leaks, high-output leaks may require more advanced interventions. Lymphangiography and embolization provide safe and effective alternatives in managing persistent leaks, highlighting the evolving role of minimally invasive techniques in complex cases.
Keywords: ymphangiography; Embolization; Thyroidectomy; Post-surgical complication; Chyloma; Chyle leak.
Citation: Book R, Tamir I, Wolf R, Gross M. Effective use of lymphangiography and embolization in chyle leak following neck surgery. J Clin Images Med Case Rep. 2025; 6(1): 3412.
Introduction
Thyroidectomy, a common head and neck procedure, varies in extent with regard to neck dissection and lymph node excision, depending on the surgical indication and clinical setting of each patient. The most common postoperative complications include bleeding, hypocalcaemia, recurrent laryngeal nerve injury, and on rare occasions, thyroid storm. Due to the potential of airway compression, surgeons are cautious regarding postoperative neck swelling, most commonly resulting from postoperative hematoma in the first few hours post-operatively. However, there may also be other delayed causes such as seroma and on rare occasions, postoperative neck abscess. While Chyle Leak (CL) from thoracic duct injury is an uncommon and serious iatrogenic complication following head and neck surgery, ooccuring in 0.5-1.4% of thyroidectomies and 2-8% of neck dissections, the highest risk of CL is actually following left lateral neck dissection [1]. This is related to the anatomy of the region, as the lymphatic system is comprised of lymphatic capillaries, vessels, nodes, ducts, and various tissues throughout the body, running parallel to blood vessels to facilitate lymph circulation [2]. The thoracic duct is the largest lymphatic vessel draining up to 75% of the body’s lymph. In an adult, the right lymphatic duct receives lymph from the right thorax, arm, and head and neck region [1]. The lymphatic system serves several crucial functions, including maintenance of the body’s fluid balance, absorption of dietary fats, and modulation of the immune system. It handles excess interstitial fluid and proteins that cannot return through blood vessels. Lymph production is dependent on many variables but it is estimated at approximately 2 millilitres per kilogram per minute, resulting in a daily output of 2 to 4 Liter [2,3]. Chyle leaks, with their loss of key components, can lead to serious problems like malnutrition, electrolyte imbalances, and fluid disturbances, thereby resulting in in primary hypoproteinemia, hyponatremia, hypokalemia, and hypocalcemia, potentially complicating primary hypovolemia due to fluid shifts. Chyle leaks can also result in leukopenia thereby increasing the risk of wound complications including delayed wound healing, infections, and sepsis [2]. It is important to identify CL as early as possible, while some may be identified intraoperatively, others are only recognized postoperatively [1]. Due to the potential significant morbidity associated with CL, leaks identified at the time of surgery should be repaired immediately. Following surgery, management of CL depends on drain output, patient comorbidities, and surgeon preference. Chyle leaks may be broadly categorized as low output (<500 mL/day) or high output (>500 mL/day), based on drain output to assist with treatment decision making. In general, low output CL can be treated effectively with conservative management, while high output CL will often respond unsatisfactorily to conservative management alone and require surgical intervention [1]. Management of these iatrogenic injuries has ranged from conservative medical management, such as minimizing dietary fat in-take, to operative intervention. Operative management has included exploration of the thoracic duct via open thoracotomy, sometimes using additional agents such as fibrin glue or tetracycline sclerotherapy [4].
Case report
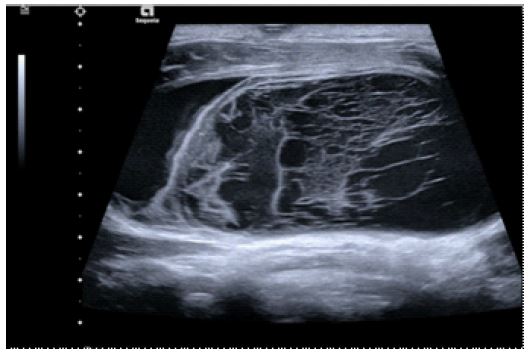
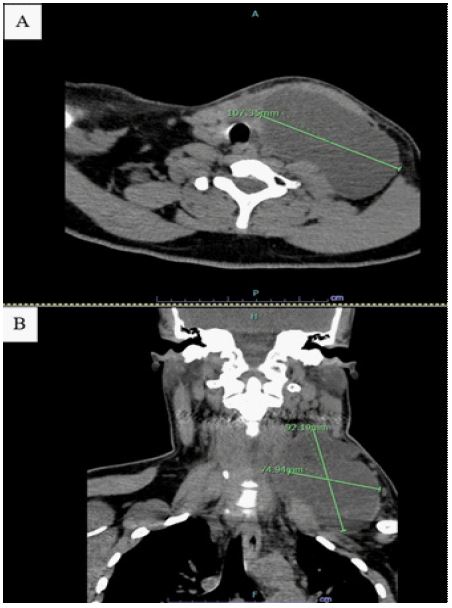
A 33-year-old woman presented for consultation to the Otolaryngology-Head and Neck Surgery Department on a referral from the Oncology Department, for evaluation of neck swelling six weeks after total thyroidectomy and left neck dissection at an outside hospital. The patient had presented to the Oncology Department for elective hospitalization for administration of post-surgical iodine treatment after pathology showed papillary thyroid carcinoma with two positive lymph nodes - T2N1M0. The patient described the swelling as gradually growing since the thyroid surgery with no associated complains. Physical examination demonstrated an enlarged, fluctuant, non-tender mass in the left neck area, with no visible erythema. On flexible fiberoptic laryngoscopy normal vocal fold movement and no compromised airway were seen. Blood laboratories showed no sign of infection, with white count of 7.4K and CRP 0.52 mg/dL. Ultrasound of the neck was performed, revealed a massive collection in the left surgical bed, with mass effect on the trachea and compression of the left jugular vein (Figure 1). Differential working diagnosis included hematoma or seroma. A Computed Tomography scan of the neck, without contrast media was performed due to the upcoming iodine treatment, demonstrated septate left neck collection (Figure 2).
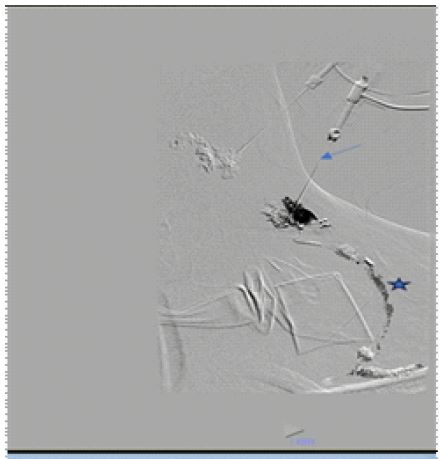
Surgical intervention: Following initial evaluation and imaging, emergent surgical intervention was decided in order to drain the collection. Under general anesthesia, an incision was made in the previous scar, revealing a thick white capsule. Following capsular incision, a large amount of straw colour fluid drained out with an impression of chyle collection. No active lymph vessels flow was seen. A drainage was left, part of the capsule was sent for histopathology evaluation, and a fluid sample was sent for biochemistry evaluation. Biochemistry evaluation revealed a high diastase 227 U/L and very high triglycerides 1763 mg/Dl. Histopathological evaluation of the capsular tissue revealed an amorphic eosinophilic material with connective tissue. The patient was admitted for observation and therapy with intravenous antibiotic treatment, octreotide therapy, Medium Chain Triglyceride (MCT) diet, and pressure dressing. Due to continuous leak and the fact that in the initial drainage there was no concrete vessel that was flowing, it was decided to try lymph vessels embolization through lymphanogiography. Lymphanogiography was done under general anaesthesia with percutaneous access to the left cervical lymph node beneath the point of suspected leakage. During the injection of Lipidol (oil-based contrast agent) a significant lymphatic leakage was visualized, and a subsequent embolization was performed using histoacryl glue, effectively stopping the CL. One week following embolization a follow up ultrasound was performed on which no collection was visualized in the left neck (Figure 3).
Discussion
Chyle leaks are a known iatrogenic injury following neck surgery, requiring the surgeon and surgical care team to be attentive and work quickly to diagnose and treat these injuries. CL that are not quickly identified or treated can lead to issues such as hypovolemia, electrolyte imbalances, malnutrition, and immunosuppression due to protein, fat, essential element, and lymphocyte loss. Initially, conservative measures are typically employed, involving bed rest with slight head elevation, dietary shifts towards nonfat/low-fat or MCT diets, subcutaneous octreotide administration, and the use of suction drainage, pressure dressings, and sclerosing agents through drains. While these conservative measures are effective for low-output CL, high-output leaks tend to respond poorly. In such cases, management options include thoracoscopic thoracic duct ligation, surgical exploration, and Thoracic Duct Embolization (TDE).
Thoracoscopic duct ligation is a less invasive alternative but still carries notable risks. CL and lymphatic fistulas are infrequent post-surgical complications, particularly after lateral cervical dissections or in patients with a history of radiotherapy [5]. Slow leaks can lead to the formation of chylous lymphoceles or “chylomas” in the subsequent weeks or months, which can be managed through percutaneous drainage, sclerotherapy, or surgical resection. Surgery is recommended for high-output leak (>500 ml/day), but this decision is subjective and depends on the patient’s clinical condition and the surgeon’s expertise. Recent developments in intranodal lipiodol lymphangiography have enabled the diagnosis and treatment of lymphatic injuries in the abdomen and thorax. In persistent cases, thoracic duct catheterization via the cisterna chyli and embolization with coils or liquid agents can be performed [6]. Lymphangiography and lymphatic interventions, such as embolization, are increasingly applied for both the diagnosis and as a minimally invasive therapy for lymphatic injuries. Lymphatic embolization has been shown to be a safe and effective method for managing CL following neck surgery. It’s important to note that the location of contrast media extravasation on lymphangiography may not always be consistent, so the embolization technique should be based on the specific location of the leak. Post-embolization, the patency of the thoracic duct may be preserved in CL that do not directly involve the thoracic duct [5]. In the case presented, a chyle leak following neck surgery was promptly identified, emphasizing the critical need for vigilance in postoperative monitoring. The initial management adhered to established protocols, incorporating conservative measures such as bed rest, dietary modifications, and the use of suction drainage. These interventions align with recommended strategies for low-output chylous leaks. However, the case took a unique turn with persistent chyle leakage, challenging the effectiveness of conservative measures. This presented an opportunity for a more in-depth evaluation of alternative interventions, such as considering the appropriateness of thoracoscopic thoracic duct ligation or embolization. Assessing the nuances of this case prompts a reflection on the existing protocols and whether, in certain scenarios, an earlier shift to more invasive interventions could be considered. The emerging techniques, like intranodal lymphangiography and catheterization with embolization, warrant exploration for their applicability and potential benefits in cases with unique challenges or atypical responses to standard conservative measures. This prompts a consideration of how the evolving landscape of lymphatic interventions could be integrated into the broader framework of managing CL, providing insights into potential advancements in treatment strategies.
Conclusion
This case underscores the importance of flexible management of chyle leaks. While conservative treatments are effective for low-output leaks, high-output leaks may require more advanced interventions. Lymphangiography and embolization provide safe and effective alternatives in managing persistent leaks, highlighting the evolving role of minimally invasive techniques in complex cases.
References
- Delaney SW, Shi H, Shokrani A, Sinha UK. Management of Chyle Leak after Head and Neck Surgery: Review of Current Treatment Strategies. Int J Otolaryngol 2017; 2017: 1-12. https://doi.org/10.1155/2017/8362874.
- Leović D, Grgić MP, Radojković IG, Blivajs I, Matoc L, et al. Management of Chyle Leak Following Head and Neck Surgery: Review of Current Treatment Strategies and Algorithmic Approach to The Treatment. Acta Clin Croat. 2022; 61: 88-95. https://doi.org/10.20471/acc.2022.61.s4.11.
- Deshmukh R, Kulkarni P, Bhutekar U, Kala A, Richhariya S, et al. Management of chyle leak in right side neck dissection: a rare case and review of literature (a case report). Pan Afr Med J. 2021; 40. https://doi.org/10.11604/PAMJ.2021.40.209.30496.
- Scott KJ, Simko E. Thoracoscopic management of cervical thoracic duct injuries: An alternative approach. Otolaryngology - Head and Neck Surgery. 2003; 128: 755-7. https://doi.org/10.1016/S0194-5998(03)00253-5.
- Kim J, Bang DH, Choi TW, Won JH, et al. Lymphangiography and lymphatic embolisation for the treatment of chyle leaks after neck surgery: assessment of lymphangiography findings and embolisation techniques. Br J Radiol. 2023; 96. https://doi.org/10.1259/BJR.20220831.
- Erdemir A, Dökdök M, Raşa K. Thoracic Duct Embolization for Postoperative Lymphatic Fistula. Case Rep Surg. 2022; 2022: 1–4. https://doi.org/10.1155/2022/7510793.