
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Diagnosing and managing villonodular synovitis in the ankle: A case report and review of the literature
Joud Boutaleb1*; Sarah Loubaris1; Basma Beqqali1; Manal El Beyeg2; Ouijdane Zamani1; Rachida Saouab1; Jamal El Fenni1
1Radiology Department, Mohammed V Military Hospital, Rabat, Morocco.
2Anatomopathology Department, Mohammed V Military Hospital, Rabat, Morocco.
*Corresponding Author : Joud Boutaleb
Radiology Department, Mohammed V Military Hospital, Rabat, Morocco.
Email: joud.boutaleb@hotmail.fr
Received : Dec 09, 2024
Accepted : Dec 27, 2024
Published : Jan 03, 2025
Archived : www.jcimcr.org
Copyright : © Boutaleb J (2025).
Abstract
This case report describes a 35-year-old male with a history of recurrent ankle sprains who presented with progressively disabling mechanical pain in the left ankle, unresponsive to analgesic treatment. Clinical examination revealed a firm, painless mass without signs of inflammation. Imaging studies including ultrasound, MRI, and CT confirmed the diagnosis of Villonodular Synovitis (VNS). A surgical biopsy confirmed the diagnosis, and the patient underwent subtotal synovectomy and mass resection. At an 8-month follow-up, there was no clinical recurrence. This report discusses the clinical, radiological, and histopathological features of VNS, its pathophysiology, and treatment strategies, emphasizing the need for early diagnosis and intervention.
Keywords: Villonodular synovitis; Ankle; MRI.
Citation: Boutaleb J, Loubaris S, Beqqali B, Beyeg ME, Zamani O, et al. Diagnosing and managing villonodular synovitis in the ankle: A case report and review of the literature. J Clin Images Med Case Rep. 2025; 6(1): 3413.
Introduction
Villonodular Synovitis (VNS) is a rare but benign pathology characterized by a pseudotumorous proliferation of the articular synovium with an unknown etiology [1]. It predominantly affects the bursae and tendon sheaths of large joints such as the knee and hip, with the ankle being an uncommon site of occurrence [2].
Case report
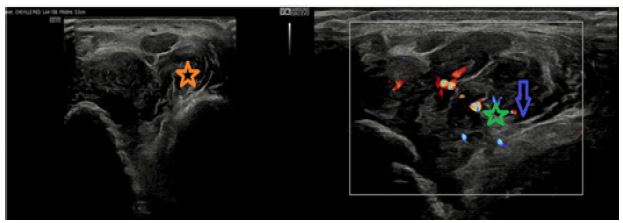
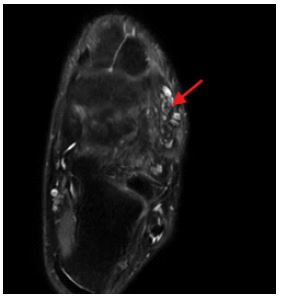
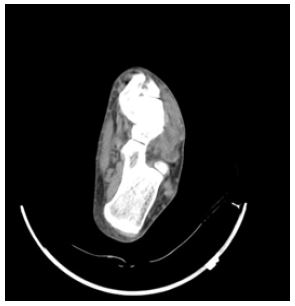
We report the case of a 35-year-old male with a history of recurrent ankle sprains who had been experiencing progressively disabling mechanical pain in his left ankle for several months, unresponsive to analgesic treatment. This clinical presentation occurred in a context of apyrexia and preserved general health. Clinical examination revealed a firm, painless mass on palpation, without inflammatory signs. Ultrasound revealed a poorly defined, hypoechoic lesion with thickened synovium containing vascularized vegetations on Doppler imaging (Figure 1). Magnetic Resonance Imaging (MRI) demonstrated a heterogeneous intra-articular mass on the lateral aspect of the ankle with lobulated contours, showing hypointensity on T1-weighted sequences and heterogeneous hyperintensity on T2-weighted sequences. The lesion measured 47×33×23 mm (HxWxT) and enhanced after contrast administration, with synovial thickening suggestive of a pseudotumoral pathology (Figures 2 and 3). Complementary CT imaging did not reveal phleboliths or calcifications (Figure 4). In the trauma department, the patient underwent a surgical biopsy via direct approach. Histopathological analysis confirmed the diagnosis of a Pigmented Villonodular synovitis (PVNS) through the identification of a tumorous proliferation consisting of monomorphic mononuclear cells with oval, finely nucleolated nuclei. Numerous multinucleated giant cells and foamy histiocytes were also observed, along with a synovial border at the periphery (Figure 5). The patient subsequently underwent mass resection through an anterolateral approach with subtotal synovectomy. At the 8-month follow-up, no clinical recurrence was noted.
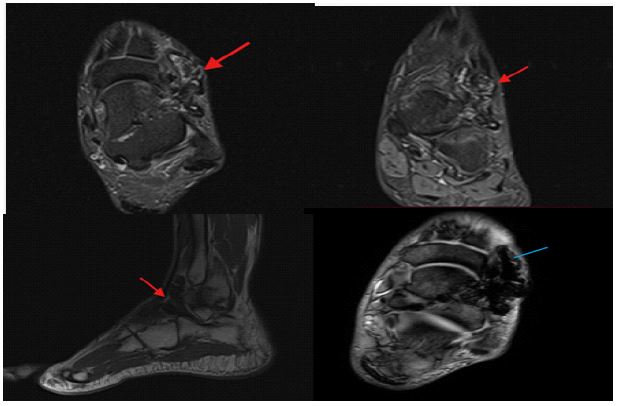
C: Sagittal T1 section demonstrating hyposignal lesion (red arrow).
D: axial T2* section showing asignal lesion (blue arrow).
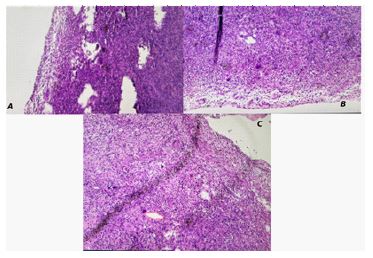
(C) Magnified histological view highlighting inflammatory infiltrates, multinucleated giant cells, and prominent synovial hyperplasia characteristic of diffuse-type tenosynovial giant cell tumor.
Discussion
First described in 1941 by Chassignac and later by Jaffe et al. [2], Villonodular Synovitis (VNS) is a rare fibrohistiocytic tumor characterized by hyperplasia of synovial villi, forming nodules. The most commonly affected joints are the knee (80%), hip (10%), and, less frequently, the ankle (5%) [3].
The etiology remains unknown; however, two pathophysiological mechanisms are proposed to explain villonodular proliferation: inflammatory and tumoral. The etiology of VNS remains unclear, with two main pathophysiological mechanisms proposed:
Inflammatory mechanism: A study analyzing genomic DNA from synovial biopsies - 20 years ago - demonstrated monoclonal proliferation, suggesting that VNS may result from a reactive inflammatory process secondary to repeated trauma or bleeding [5].
Tumoral mechanism: Fletcher et al. proposed the more widely accepted hypothesis of monoclonal tumoral proliferation, with 35% of pathological cells displaying trisomy 7 [2]. Recent studies have also identified a 1p13 and 2q37 translocation, leading to overexpression of CSF-1, which contributes to cellular proliferation [3].
Two forms of VNS are recognized:
Localized form: This form typically presents with mechanical discomfort, often accompanied by a palpable, progressive developing mass. Such masses are more evident in superficial regions, as observed in our patient [6].
Diffuse form: This is characterized by joint effusion, resulting in restricted mobility. Late presentations may involve synovial lesions extending to adjacent bone and soft tissues. Recurrent effusions, common in diffuse VNS, can mimic rheumatoid arthritis. However, the presence of intermittent or persistent hemarthrosis should prompt reevaluation of the diagnosis [7,8].
Clinical and radiological signs: The clinical presentation of VNS is nonspecific and sometimes misleading, which explains the delay of several months before a final diagnosis is established. The most common presentation is a palpable monoarticular swelling causing progressively worsening functional impairment [9].
Standard X-rays are typically normal but may show bone erosions at advanced stages due to the destructive nature of VNS.
In localized forms, ultrasound may reveal a hypoechoic lesion containing vascularized vegetations on Doppler imaging, potentially accompanied by joint effusion [11]. MRI is the imaging modality of choice and demonstrates pathognomonic features of multiple synovial lesions [10], including:
• Hypointense areas on all sequences due to hemosiderin deposition.
• Hypointense T1 and hyperintense T2 areas consistent with hypervascularized inflammatory lesions.
• Hyperintense T1 and T2 areas corresponding to lipid deposits and foamy cells.
• Histological analysis remains essential for confirming the diagnosis.
Evolution and treatment: The regional progression of VNS is slow, with extension to the entire synovium, adjacent bone, and soft tissues. Untreated localized VNS may progress to a diffuse form, highlighting the importance of early and appropriate treatment. Treatment is not yet standardized but primarily involves meticulous surgical synovectomy, aiming for complete removal. In diffuse forms, total synovectomy should be supplemented with bone curettage [12].
Some authors advocate synoviorthesis (isotopic or osmium-based) in cases of incomplete synovectomy. Others suggest anti-tumor necrosis factor alpha (anti-TNF-α) therapy for patients refusing conventional treatments, though its efficacy remains debated [13]. The long-term prognosis depends on lesion extent at diagnosis, site, and quality of surgical excision. Localized forms generally resolve after complete excision, with an almost negligible risk of recurrence [14].
Conclusion
Localized VNS primarily affects the knee (75% of cases), followed by the hip and, rarely, the ankle. Clinical presentation is often nonspecific. MRI remains the key diagnostic and follow-up tool for this pathology. The final diagnosis relies on histological examination of synovial biopsies or surgical specimens.
References
- Benabbouha A, Basinga J, Anteri I, Jaafar A. Villonodular synovitis of the ankle, a rare localization : A case report.
- Cupp JS, Miller MA, Montgomery KD, et al. Translocation and expression of CSF1 in pigmented villonodular synovitis, tenosynovial giant cell tumor, rhumatoid arthritis and other reactive synovitides. Am J Surg Pathol. 2007; 31: 970-6.
- Fletcher JA, Henkle C, Atkins L, Rosenberg AE, Morton CC. Trisomy 5 and trisomy 7 are nonrandom aberrations in pigmented villonodular synovitis: Confirmation of trisomy 7 in uncultured cells. Genes Chromosomes Cancer. 1992; 4: 264-6.
- Localised villonodular synovitis of the ankle with bone damage M. Benchakroun · M. Boussouga · S. Kadi J. Boukhris · A. Jaafar.
- Sakkers RJ, de Jong D, van der Heul RO. X-chro- mosome inactivation in patients who have pigmented villonodular synovitis. J Bone Joint Surg Am. 1991; 73: 1532-6.
- Duriez IF, Orcel P, Prier A, Kaplan G. Villonodular synovitis of the wrist: A case report Réa’ Rfzinn Ma/Os/Mat-tic. 1986 53: 655-6.
- Cheng XG, You YH, Liu W, et al. MRI features of pigmented villonodular synovitis (PVNS). Clin Rheumatol. 2004; 23: 31-4.
- Flandry FC, Hughston JC, Jacobson KE, et al. Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop. 1994; 300: 183-92 .
- Wagner ML, Spjut HJ, Dutton RV. Polyarticular pigmented villonodular synovitis Am J Roentgenol. 1981; 136: 821-3.
- Hernigou PH, Marichez M, Voisin MN, et al. The contribution of magnetic resonance imaging in the assessment of pseudotumoral villonodular synovitis of the knee. Rev Chir Orthop. 1990; 76: 218-21.
- Flipo RM, Chastanet P, Duquesnoy B. Imaging pigmented villonodular synovitis. Presse Med. 1993; 22: 591-4.
- Dines JS, DeBerardino TM, Wells JL, et al. Long-term follow-up of surgically treated localized pigmented villonodularsynovitis of the knee. Arthroscopy. 2007; 23(9): 930-
- Sharma V, Cheng EY. Outcomes after excision of pigmented villonodular synovitis of the knee. Clinical Orthopaedics and Related Research. 2009; 467(11): 2852- 2858.
- Ogilvie-Harris DJ, Mc Lean J, Zarnett ME. Pigmented villonodular synovitis of the knee: Results of total arthroscopic synovectomy, partial arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am.1992; 74(1): 119-23.