
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Immediate effect of robotic therapy using Armeo® on temperature distribution in the upper limbs of patient with stroke sequelae
Fábio Marcon Alfieri1*; Daniela Mitiyo Odagiri Utiyama2; Linamara Rizzo Battistella1,3
1Clinical Research Center of the Institute of Physical Medicine and Rehabilitation, Hospital das Clínicas HCFMUSP, Faculty of Medicine, University of São Paulo, São Paulo, Brazil.
2Physiotherapist at the Institute of Physical Medicine and Rehabilitation, Hospital das Clínicas HCFMUSP, Faculty of Medicine, University of São Paulo, São Paulo, Brazil.
3Department of Legal Medicine, Medical Ethics, Social Medicine, and Occupational Medicine, Faculty of Medicine FMUSP, University of São Paulo, São Paulo, Brazil.
*Corresponding Author : Fábio Marcon Alfieri
Clinical Research Center of the Institute of Physical Medicine and Rehabilitation, Hospital das Clínicas HCFMUSP, Faculty of Medicine, University of São Paulo, São Paulo, Brazil.
Email: fmalfieri@gmail.com
Received : Dec 02, 2024
Accepted : Dec 30, 2024
Published : Jan 06, 2025
Archived : www.jcimcr.org
Copyright : © Alfieri FM (2025).
Abstract
Currently, the use of robotic therapy is being increasingly used for the rehabilitation of individuals with stroke sequelae. This case report describes a patient who underwent a single session of robotic therapy, being evaluated using thermography, a painless method that evaluates the distribution of skin temperature. The article shows changes in temperature after an exercise session performed using a robotic device and discusses the possibility of this evaluation technique (thermography) in patients with stroke undergoing different rehabilitation techniques such as robotic training.
Keywords: Stroke; Robotic devices; Rehabilitation; Thermography; Evaluation.
Citation: Alfieri FM, Utiyama DMO, Battistella LR. Immediate effect of robotic therapy using Armeo® on temperature distribution in the upper limbs of patient with stroke sequelae. J Clin Images Med Case Rep. 2025; 6(1): 3414.
Introduction
The use of robotic devices has been useful in the rehabilitation process of patients with the sequelae of cerebrovascular accident or stroke [1]. A systematic review showed that training with a robotic device can significantly improve the motor function of the upper limbs and activities of daily living in patients with stroke [2]. This probably occurs due to the fact that the systematic movement of the affected limbs, which is essential in rehabilitation, it is facilitated and encouraged during robotic training [3]. An example of this type of device is the Armeo® system, which is a robot intended for motor rehabilitation of the upper limb and which works with upper support for the arm, lower support for the forearm and a pressure-sensitive handle. The equipment has adjustments to align the exoskeleton with the joints and has an interactive program that controls the arrangement and provides visual feedback through a screen. It has the advantage of allowing work in an interactive, repetitive and individualized manner with a focus on training specific tasks using defined protocols [4]. Regarding the immediate effect of robotic interventions in patients with stroke sequelae on the distribution of body temperature assessed by thermography, one study found that a patient undergoing robotic therapy using the G-EO SystemTM device managed not only to increase skin temperature, but reduce the differences between the plegic and healthy sides [5]. Thermography is useful in measuring the distribution of body temperature in patients with stroke [6] and also to identify changes in temperature after a single session of exercise, for example, in patients with amputation sequelae [7] or with vascular impairments [8]. How, at least to our knowledge, there are no studies on the use of thermography as an evaluation method in patients who have undergone physical rehabilitation using a robotic device for upper limbs. This case report aimed to verify the temperature distribution of the upper limbs of an individual with sequel to stroke submitted to a single session of robotic rehabilitation using Armeo®.
Case presentation
GDS, 29 years old, with completed high school, married, born in Lavras da Manga do Ceara, from Guarulhos in the state of São Paulo, worked in cargo transport. He is dominant on the right side and diagnosed with disproportionate spastic complete hemiparesis with brachial predominance on the right (October 2022). As for etiology, it was secondary to arteriovenous malformation radioablation (on 03/01-07/01/2022). He presents hearing loss with hemianopia on the right. The patient came to the institution with a previous history of external follow-up at another institution with a multidisciplinary team in which he underwent physiotherapy, speech therapy, occupational therapy and acupuncture. He arrived at the Institute of Physical Medicine and Rehabilitation of the Hospital das Clínicas of the Faculty of Medicine of the University of São Paulo (IMREA-HCFMUSP) with modified independence for activities of daily living and performed some self-care activities under supervision or with preparation of third parties despite having the ability to perform independently. He had an unstable gait with a tendency to invert the ankle during stance, with a risk of sprain. Patient and wife already noticed cognitive changes in relation to memory and occasional semantics and presented the FIM-Functional Independence Measure 9 of 116 points. The patient underwent hospitalization for brain injury rehabilitation, remaining with a companion during the entire hospitalization. In the rehabilitation sessions, motor training was carried out focusing on walking on uneven terrain, dynamic balance, dual tasks and progressive load increase, greater participation in fine motor activities using the right upper limb as support, and global cognitive stimulation. The patient always showed good motivation and effort, with no complications during hospitalization, with a notable improvement in mood and cognition as he noticed an improvement in functionality. Regarding gait, the patient started using an ankle stabilizing orthosis with an improvement in his gait pattern, even progressing to community walking in an external environment, without the need for aids. He also performed isokinetic strengthening with Cybex of the knee with excellent performance. Before hospitalization, in march/2023, he underwent the first application of botulinum toxin, but the patient reported progress with loss of functionality in the right upper limb (no longer able to perform functional finger flexion and elbow flexion in functional range). And, due to this, baclofen medication was started, which together with kinesiotherapy can provide gains in range in the right upper limb and improvement in movements such as pronation and supination with greater participation in fine motor activities. The GDS patient presents great use of therapies, with no indication for further hospitalization, with a proposal for outpatient follow-up and maintenance therapies in the community. As an outpatient, the patient underwent 15 sessions of Armeo® with the aim of promoting the functionality of the right upper limb, improving perception and control of it, as well as dissociation of movements according to the demands of the tasks. With the objective of evaluating the effect of carrying out a single robotic training session using the Armeo® device on the distribution of skin temperature, this case study was carried out. To evaluate this single session, the training protocol was placed on Armeo® with the aim of improving motor control of the left upper limb with a game of balloons, pirates, brick breaking (shoulder), high flying (elbow), Hocokart (forearm), treasure island, helicopter, cleaning. Each game lasts 5 minutes and has a medium to hard difficulty level. Before and after this single robotic training session, a skin thermometry examination was carried out using infrared thermography in a room next to the therapeutic space where the robotic device was located. The room had the windows and curtains closed, in order to prevent any type of external light from entering it and the relative humidity was 47% in the first image taking and 44% in the second and with a temperature of 24.5°C and 23.8° respectively. As the conditions for this type of examination must be standardized, measures reported in the literature were adopted [10-15]. The patient was instructed not to take hot baths or showers, apply creams, powders or perform vigorous exercise before the evaluation. He must have fasted for up to two hours and could not have ingested stimulants, substances containing caffeine or nasal decongestants, drinks containing alcohol and could not have smoked. The volunteer was asked to remain bare in the room with their torso and upper limbs. The patient was instructed to remain standing at a distance of 2 meters from the infrared sensor and 0.4 m from the wall. The entire skin temperature assessment procedure obtained by thermographic assessment followed the criteria adopted and recommended in the literature [10-14]. The thermal images were captured by an infrared sensor, brand FLIR T450SC. These images were obtained in views: anterior and posterior. The images were analyzed by FLIR Tools® software and included the right and left sides of the arms, forearm, chest and spine. The average temperature was measured in degrees Celsius in each ROI (region of interest). The ROI were rectangles determined by anatomical landmarks, named: 1-forearm: distal forearm and cubital fossa; 2-Arm: cubital fossa and axillary line, 3-abdomen: (and lumbar region): xiphoid process and 5 cm below the navel, 4-chest (upper back): nipple line and upper edge of the sternum. This evaluation has already been described and carried out in a previous study [10]. The evaluations were carried out before, immediately after the end of the robotic therapy and 10 minutes in the afternoon after the therapy that was carried out with the Armeo® system. The temperature distribution between the upper limbs is shown in (Table 1). When checking the temperature on both sides, on average, it was 32.2°C before the single Armeo® session and increased to 33.0°C after, with an increase of 0.8°C considering both sides. When checking the difference between the plegic and healthy sides, it was noted that the arm (in the anterior view) had a difference of 0.8°C. However, after the robotic training session, this difference disappeared, leaving the sides completely symmetrical in relation to the temperature difference. However, even after the intervention, the forearm in the posterior view had an increase in the difference between the sides, going from 0.4° to 0.7°, that is, both temperatures at a level that indicates some type of change 16. In general, the healthy side presented 32.3 before the intervention and 33.1 after the intervention, increasing by 0.8°C. The plegic side presented 32.0 before the intervention and 32.9 after the intervention, increasing by 0.9°C.
Table 1: Skin temperature (in °C) of the forearm and upper arm before and after the single session of robotic therapy using Armeo®.
| Baseline | Difference between healthyand plegic sides | Immediate | Difference between healthyand plegic sides | Difference betweenbaseline and immediate | ||
|---|---|---|---|---|---|---|
| Anterior view | Heathy forearm | 32.8 | 0.1 | 33.4 | 0.3 | 0.6 |
| Plegic forearm | 32.9 | 33.7 | 0.8 | |||
| Healthy arm | 33.4 | 0.8 | 34.4 | 0.0 | 1 | |
| Plegic arm | 32.6 | 34.4 | 1.8 | |||
| Posterior view | Heathy forearm | 31.8 | 0.4 | 32.3 | 0.7 | 0.5 |
| Plegic forearm | 31.4 | 31.6 | 0.2 | |||
| Healthy arm | 31.5 | 0.1 | 32.4 | 0.2 | 0.9 | |
| Plegic arm | 31.4 | 32.2 | 0.8 |
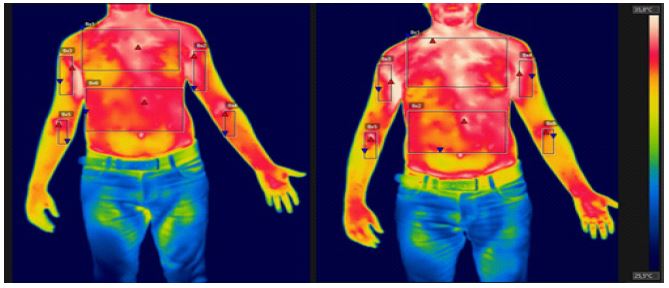
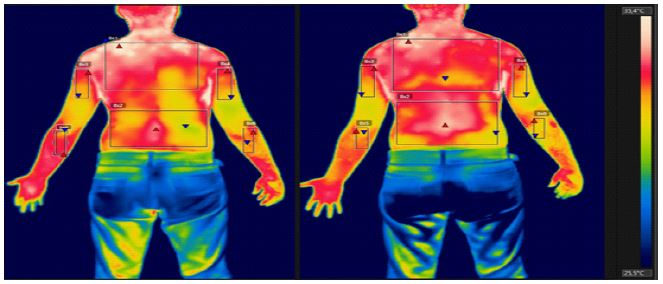
Table 2: Skin temperature (in degrees Celsius °C) of the spine before and after the single session of robotic therapy using Armeo®.
| Baseline | Immediate | Difference | |
|---|---|---|---|
| Anterior chest Posterior chest Abdomen Low back region |
33.4 32.3 33.1 31.2 |
34.7 33.2 34 33 |
1.3 1.1 0.9 1.9 |
The temperatures related to the trunk are shown in (Table 2). It can be seen that there is an increase in temperature in both the anterior and posterior regions, with an average increase of 1.3°C after a single exercise session using a robotic device.
Figures 1 and 2 show the temperature distribution in the front and back views.
In this case report, the temperature data show that in relation to the structures evaluated, only the arm in the anterior view before the robotic intervention and the forearm in the posterior view before and after the single exercise session, showed important differences. This is because it is known that individuals, when they present a difference above 0.4°C, may present some type of change [16]. The patient in this report has stroke sequelae and, therefore, the plegic side is expected to be colder [6]. However, a fact that needs to be highlighted is the increase in temperature after the robotic training session. This increase occurred both on the healthy side and on the plegic side and in the trunk region, both in the anterior region, thorax and abdomen, and posteriorly, in the thoracic and lumbar spine region. In addition, this probably reflects the increase in muscle recruitment through exercise, which may have indirectly increased blood perfusion and, therefore, skin vascularization [14]. It is worth noting that perhaps the contact of the body with the chair may have interfered with the increase in temperature in the posterior region, however it is important to highlight that the anterior region, which did not have this contact, also had a significant increase in temperature, probably showing the muscular action of this region during exercise. Therefore, it is believed that thermography can be a useful instrument to detect this type of change in skin temperature, as seen in other case reports also carried out with robotic devices [5], treadmills associated with virtual reality [7] or a simple circuit ergometric [8].
Conclusion
A single case and the evaluation after a single session of robotic intervention cannot generalize the data on thermoregulation after exercise performed on a robotic device. However, it leads to the belief that this type of exercise, which is playful and pleasant for the patient, also exerts important physiological changes such as thermoregulation. Therefore, prospective studies can show the effects of this type of rehabilitation, as well as other models associated or not, such as conventional therapy on the thermal regulation of individuals with various types of functional changes.
Compliance with ethical standards: No conflicts of interest. Informed consent was taken from the patient for the publication of the case report. No funding was provided for this manuscript. There are no financial interests to disclose by the authors.
References
- Poli P, Morone G, Rosati G, Masiero S. Robotic technologies and rehabilitation: new tools for stroke patients’ therapy. Biomed Res Int. 2013; 2013: 153872.
- Yang X, Shi X, Xue X, Deng Z. Efficacy of Robot-Assisted Training on Rehabilitation of Upper Limb Function in Patients With Stroke: A Systematic Review and Meta-analysis. Arch Phys Med Rehabil. 2023; 104(9): 1498-1513.
- Volpe BT, Krebs HI, Hogan N, Edelstein OL, Diels C, et al. A novel approach to stroke rehabilitation: robot-aided sensorimotor stimulation. Neurology 2000; 54: 1938-1944.
- Yáñez-Sánchez A, Cuesta-Gómez A. Efectividad del dispositivo Armeo ® en la rehabilitación del miembro superior en pacientes que han sufrido un ictus. Revisión de la bibliografía [Effectiveness of the Armeo® device in the rehabilitation of the upper limb of stroke’s patients. A review of the literature]. Rev Neurol. 2020; 70(3): 93-102.
- Alfieri FM, Dias CDS, Dos Santos ACA, Battistella LR. Acute Effect of Robotic Therapy (G-EO System™) on the Lower Limb Temperature Distribution of a Patient with Stroke Sequelae. Case Rep Neurol Med. 2019; 2019: 8408492.
- Dias CDS, Alfieri FM, Dos Santos ACA, Battistella LR. Whole-body thermographic assessment of patients with stroke sequelae who report temperature differences between the sides. Thermology International 2022; 32: 14-19.
- Alfieri FM, Dias CDS, Utiyama DMO, Ayres DVM, Battistella LR. The Immediate Effect of Exercising in a Virtual Reality Treadmill (C-Mill) on Skin Temperature of a Man with Lower Limb Amputation. Case Reports in Vascular Medicine. 2023; 1-5.
- Dias CDS, Alfieri FM, Andrade VCS, Battistella LR. Immediate effect of a single cycle ergometry session on skin temperature of women with and without varicose veins: a case report. Thermology International. 2021; 31: 11-18.
- Riberto M, Miyazaki MH, Jucá SSH, Sakamoto H, Pinto PPN, et al. Validação da Versão Brasileira da Medida de Independência Funcional. Acta Fisiátr. [Internet]. 9º de agosto de 2004 [citado 18º de setembro de. 2024; 11(2): 72-6.
- Marins JC, Fernandes AA, Cano SP, Moreira DG, da Silva FS, et al. Thermal body patterns for healthy Brazilian adults (male and female). J Therm Biol. 2014; 42: 1-8.
- Szentkuti A, Kavanagh HS, Grazio S. Infrared thermography and image analysis for biomedical use. Periodicum biologorum 2011; 113(4): 385-92.
- Ring EFJ, Ammer K. The Technique of Infrared Imaging in Medicine. Thermology international. 2000; 10(1): 7-14.
- Ring EF, Ammer K. Infrared thermal imaging in medicine. Physiol Meas. 2012; 33(3): 33-46.
- Fernández-Cuevas I, Bouzas Marins JC, Arnáiz Lastras J, Gómez Carmona, PM, Piñonosa Cano S, García-Concepción MÁ & Sillero-Quintana M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Physics & Technology. 2015; 71(0): 28-55.
- Alfieri FM, Battistella LR. Body temperature of healthy men evaluated by thermography: A study of reproducibility. Technol Health Care. 2018; 26(3): 559-564.
- Vardasca R, Ring EFJ, Plassmann P, Jones CD. Thermal symmetry of the upper and lower extremities in healthy subjects. Thermol Int. 2012; 22(2): 53-60.