
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Study - Open Access, Volume 6
The early initiation of treatment of overweight and obesity with liraglutide in patients with different obesity phenotypes
*Corresponding Author : Štefan Farský
Dom srdca Martin, National CVD Prevention Coordinator of the European Association of Preventive Cardiology for Slovakia.
Email: farsky@za.psg.sk
Received : Dec 07, 2024
Accepted : Dec 30, 2024
Published : Jan 06, 2025
Archived : www.jcimcr.org
Copyright : © Farský S (2025).
Abstract
Early pharmacological initiation in treatment of (pre)obesity and obesity in various obesity phenotypes becomes the important point of the health care system focused on weight loss and consequent health improvement. The European Association for the Study of Obesity has published an important new paper in Nature Medicine outlining an updated framework on the diagnosis, staging, and management of obesity in adults, emphasizing understanding obesity as an adiposity-based chronic disease. The framework focuses on comprehensive, personalized evaluation and management strategies with the objective of improving health. Despite the fact that (pre)obesity is defined as a chronic disease and is easily diagnosed in patients, it is often overlooked and untreated. With new pharmacological options for the treatment of obesity, such as liraglutide presented in the case reports, the possibility of treating obesity as a primary clinical problem opens up in outpatient clinics. We present 2 case reports of patients treated with liraglutide in our cardiology clinic with different phenotypes of obesity, class of obesity and at different stages of the disease, with an emphasis on results reflecting not only a reduction in body weight, but an improvement in the overall health of the patients. Despite their different BMI and different phenotype, according to the Edmonton Obesity Grading System, both are in stage 2 obesity, suitable for pharmacotherapy and management in outpatient clinic care.
Keywords: Pre-Obesity; Obesity classification; Liraglutide; Obesity phenotypes.
Citation: Farský S. The early initiation of treatment of overweight and obesity with liraglutide in patients with different obesity phenotypes. J Clin Images Med Case Rep. 2025; 6(1): 3415.
Introduction
The European Association for The Study of Obesity (EASO) has published an important new document in Nature Medicine [1], outlining an updated framework for the diagnosis, staging, and management of obesity in adults, emphasizing an understanding of obesity as an Adiposity-based Chronic Disease. This shifts the diagnosis of obesity from anthropometric BMI thresholds to considering the role of fat tissue distribution and function in the severity of the disease.
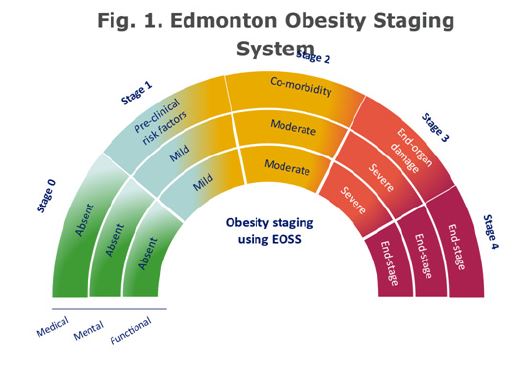
The stages of obesity according to the Edmonton Obesity Staging System (EOSS)
EASO has proposed establishing the diagnosis of obesity based on the accumulation of a large amount of fat or the presence of abnormal fat (anthropometric component), along with an analysis of existing clinical factors having potential impact on health status (clinical component). The clinical component includes the assessment of obesity-related health complications and metabolic risk factors, evaluation of functional status, mental health, and eating behavior disorders. Following the establishment of the diagnosis of obesity, the next step is to determine the stage of this chronic, relapsing disease based on the severity of health, mental, and functional complications according to the Edmonton Obesity Staging System (EOSS) [2-4], (Figure 1). This determination allows for a dynamic view of obesity as a chronic, progressive pathological process that can transition from a relatively asymptomatic stage to a stage where abnormal or large fat accumulation is accompanied by health impairment, potentially progressing to a disabling or life-threatening disease stage. The new document from EASO emphasizes comprehensive and personalized strategies for assessing and managing patients with obesity in order to improve their health status. The current anthropometric approach, for example, excludes the indication for pharmacotherapy or bariatric surgery in patients with significant (pre)obesity impact on their health status, even if their BMI values are relatively low. The expert panel now recommends early initiation of obesity treatment in patients with a BMI ≥25 kg/m2, whose waist-to-height ratio is above 0.5, and who also have present health, functional, or psychological complications. The goal of managing patients with obesity should therefore shift from mere body weight reduction to improving complication status and enhancing quality of life. The current anthropometric definition of obesity also provides limited information on the risk and potential impact of the disease on individual patients, necessary for choosing a therapeutic plan and monitoring treatment outcomes. According to the new disease staging classification, treatment intensification can be achieved for patients who already have health problems related to obesity. While lifestyle change interventions and searching for additional risk factors are recommended for managing patients in stage 1 EOSS (with the presence of subclinical risk factors), for managing patients in stage 2 EOSS with existing comorbidities, psychological symptoms, or functional limitations, initiation of obesity treatment including behavioral, pharmacological, and surgical alternatives is recommended in addition to comorbidity management [2].
Obesity phenotypes
Obesity is a disease with a clinical presentation consisting of various phenotypes. BMI, as an anthropometric criterion for the diagnosis of (pre)obesity, does not reflect the entire complexity of the disease, arising from different distributions of adipose tissue and the degree of its dysfunction, nor does it consider the presence of associated conditions. In a clinical setting, in addition to BMI, we should focus on quantifying adiposity (body composition with a focus on the proportion of total fat and muscle mass, for example, using BioImpedance Analysis (BIA), distribution of adiposity (subcutaneous, visceral, and ectopic fat depots measured through waist circumference, BIA, and imaging methods). Furthermore, it is necessary to focus on the functional state of adiposity (measuring levels of adipokines and inflammatory markers) and complications associated with adiposity (presence and severity of health, mental, and functional complications according to the Edmonton Obesity Staging System (EOSS) stages) [5]. Currently, the four basic metabolic phenotypes of obesity are categorized according to the criteria listed in (Table 1) [6,7]. The threshold for waist circumference in men ≥102 cm and in women ≥88 cm, regardless of BMI, is used to define abdominal obesity. An even better predictor of increased cardiometabolic risk is the waist-to-height ratio with a threshold of 0.5 [8]. Metabolically Healthy (Pre)Obesity (MHO) and Metabolically Unhealthy (Pre)Obesity (MUO) are the most prevalent phenotypes in patients with BMI >25 kg/m2, with the main difference between them being changes in fat distribution. The healthier MHO phenotype is less common in the European population (prevalence approximately 10-30%). These individuals are typically younger, female, physically active, and have a good nutritional profile. Patients with the MUO phenotype have a larger waist circumference and a higher proportion of visceral fat, signs of metabolic syndrome, and dysfunctional, pro-inflammatory, and hypertrophic adipose tissue, or its ectopic deposits in the liver or skeletal muscles. While weight loss is recommended for patients with the MHO phenotype to maintain a favorable cardiometabolic profile (and to prevent transition to MUO), weight loss is the cornerstone of clinical management for the MUO phenotype [7]. Sarcopenic Obesity (SO) is characterized by a low proportion of skeletal muscle mass. For patients with SO, a hypocaloric diet with increased protein content (1.2-1.4 g/kg of body weight to support muscle mass) is recommended [7]. Metabolically Unhealthy Mormal Weight (MUNW) represents a phenotype whose recognition is often insufficient. This is due to the difficulty in recognizing increased visceral adiposity and imbalance in the ratio of fat to muscle mass. Also, these patients may not meet typical anthropometric obesity characteristics. They are mostly older individuals with a sedentary lifestyle and a low volume of gluteofemoral fat. The overall proportion of adipose tissue is usually lower, and their treatment strategy should focus on ectopic fat deposits (e.g., in the liver) and improving overall metabolic health. From a psychological perspective, we can also discuss various psychological-behavioral phenotypes associated with obesity. Among the psychological parameters for identifying individual phenotypes are:
• Dependence or sensitivity to reward,
• Measure of cognitive control in coordinating behavior,
• Mood and emotional disorders [9].
While this type of phenotyping extends beyond the scope of routine outpatient management of patients with obesity, it allows us to link the definition of obesity with the presence of risky psychological factors in thinking and emotions [10]. These disorders primarily lead to “overeating” beyond actual needs and, overall, inappropriate eating and exercise habits. The most common poor habits related to “overeating” for psychological reasons include:
• External triggers prompting overeating (e.g., food availability, watching television during meals, large portions).
• Internal emotional triggers prompting overeating (e.g., stress, increasing comfort).
• Internal cognitive triggers prompting overeating (e.g., black-and-white, either-or thinking).
• Unconscious automatic eating (e.g., speed of eating, various degrees of hunger and satiety).
• Lack of self-care (e.g., lack of self-control on autopilot, lack of mindfulness, self-compassion).
• Psychologists further assess lifestyle with regard to quality of life, body image, overcoming stigmatization, sleep disorders, and other issues leading to overeating [10].
The most common dietary errors include:
• Inappropriately high energy utilization in the diet.
• Inappropriate composition of the diet.
• Inappropriate eating regimen, timing of individual portions.
• Inappropriate drinking habits.
The most common poor exercise habits include:
• Minimal physical activity, both active and routine.
• Inappropriate physical activity.
• Sedentary lifestyle.
Based on the analysis of psychological triggers for overeating, dietary and exercise habits, a specialist collaborates with the patient to establish gradual and realistic goals in specific areas of lifestyle [10]. A key step in managing patients with obesity is to assess their motivational readiness for lifestyle change and weight reduction. It is important to initiate effective intervention with a patient who, according to the behavior change model, is in the “ready for change” phase. In the readiness phase, the individual intends to take necessary steps in their behavior in the near future (usually within two weeks). They are ready for change and require counseling, social support, and assistance [4].
Liraglutide in the treatment of obesity and reduction of cardiovascular (CV) and metabolic risk
GLP-1 (glucagon-like peptide 1) is an incretin hormone produced by L-cells in the intestine and in the hypothalamus. Liraglutide, an analog of human GLP-1, at a dose of 3.0 mg/day, is indicated for the treatment of obesity [11]. Specifically, liraglutide regulates appetite by increasing the feeling of fullness and satiety while simultaneously reducing hunger and the desire to consume more food [12]. The anticipated average weight loss in early responding patients after 1 year of treatment is 11.2% of their baseline body weight. Additional cardiometabolic benefits of liraglutide include:
• Improvement in glycemic parameters.
• Average reduction in waist circumference by 8.2 cm after 1 year of treatment.
• Lowering of blood pressure.
• Reduction in hs CRP levels.
• Improvement in lipid profile [11].
In adults with high CV risk and concurrent overweight or obesity, treatment with liraglutide significantly reduced visceral adipose tissue by 12.49%. Reduction in visceral fat may also be one of the mechanisms contributing to the positive cardiovascular effect of liraglutide [13]. In the LEADER trial (a type of CVOT study), liraglutide demonstrated a reduction in the risk of major CV events in patients with type 2 diabetes. The anticipated mechanism of action mainly involves slowing the progression of atherosclerotic vascular disease, reducing the amount of organ fat, and slowing the development of subsequent fibrosis in individual organs, including the myocardium [14].
Our experience and case studies
So far, we have treated 65 patients with obesity and concomitant cardiovascular diseases or with elevated cardiovascular risk without apparent cardiovascular disease in our outpatient clinic. The average duration of treatment was 3 months, sometimes treatment was interrupted and then reinitiated. The average dose of liraglutide was 2.4 mg/day, and we did not observe any significant side effects.
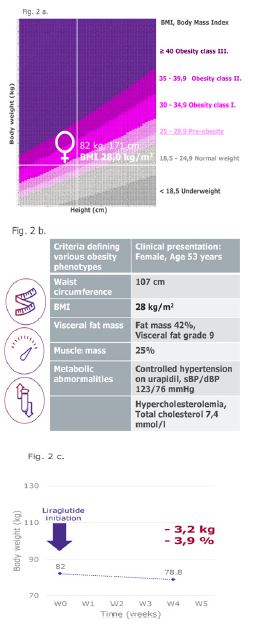
Female patient with pre-obesity in 2nd stage of the disease
An example of a situation where we might not initially consider initiating obesity pharmacotherapy in routine practice (based on BMI criteria) is a patient who meets the definition of pre-obesity (historically “overweight”) but not obesity. However, after considering her overall health status and classification according to EOSS, she is already in the 2nd stage of the disease, making obesity pharmacotherapy indicated for her. This concerns a 53-year-old patient with a history of cholelithiasis, hysterectomy for fibroids, retinal detachment, and repeated lumbar spine surgeries. Her BMI of 28 suggests pre-obesity (Figure 2a), while her waist circumference of 107 cm (Figure 2b) indicates abdominal obesity, and a waist-to-height ratio of 0.62 represents high cardiovascular risk. Body composition analysis using bioimpedance confirms an increased fat mass of 43%, with the visceral fat mass within normal range. The muscle mass ratio of 25% of body weight is at the lower limit of normal for women, not yet indicative of sarcopenic obesity. From a cardiometabolic perspective, arterial hypertension is already present, currently well controlled with urapidil 60 mg 2x1 p.o. (blood pressure value 123/76 mmHg), and hypercholesterolemia (total cholesterol level is 7.4 mmol/l). From a metabolic phenotyping standpoint, we classify the condition as Metabolically Unhealthy (pre)Obesity (MUO). In terms of determining the stage of obesity according to EOSS, the patient exhibits developed chronic comorbidities, without psychological symptoms, with moderately severe functional limitations, thus classified as stage 2. Her habits leading to “overeating” include consuming something sweet after every meal (she mentioned feeling “shaky” for something sweet after a regular meal), indicating a lack of respect for the feeling of fullness and an internal emotional trigger aimed at increasing internal comfort. The patient herself intentionally sought out our clinic for obesity treatment, indicating her readiness for change. Together, we created a treatment plan that included dietary measures, an exercise plan (involving rowing and cycling 3 times a week for 1 hour each), and we added liraglutide to the treatment with a gradual dose escalation plan to 3.0 mg/day. After just 4 weeks of liraglutide treatment with a dose escalation from 0.6 mg to 2.4 mg/day, we observed an excellent therapeutic effect (Figure 2c). In addition to a decrease in body weight of 3.2 kg (i.e., -3.9% from the original weight), a significant cardiometabolic benefit was the reduction in waist circumference by 3.5 cm. The patient subjectively perceived the effects of the treatment, describing how liraglutide therapy helped reduce her appetite, especially for sweets, which she was unable to resist before. The patient is motivated, adhering to the prescribed diet and exercise plan, continuing with further treatment, and liraglutide dose escalation. The urapidil dose was reduced to 2x30 mg.
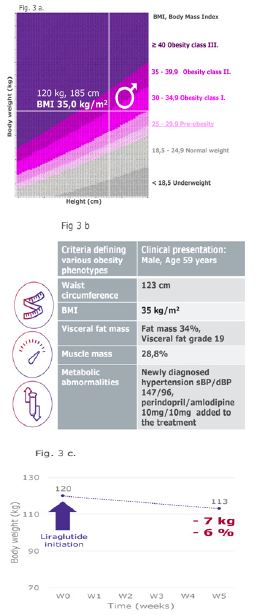
A patient with class 2 obesity at the time of transition to stage 2 of the disease
Another typical example from practice is an obese patient who has not previously had obesity-related comorbidities and whose obesity has been managed by repeated attempts to change lifestyle without much success. However, the progression of this progressive disease continued, and thus, in addition to treating comorbidity (arterial hypertension), we also indicated obesity treatment with pharmacotherapy. This is a 59-year-old patient with a history of first-degree obesity since 2013, with no other diseases. He scheduled an appointment with our clinic due to recurrently elevated blood pressure, which he attributed to stress from a new job (located away from his residence, returning home only on weekends). His current BMI was 35, classifying him as having second-degree obesity (Figure 3a), with a waist circumference of 123 cm (Figure 3b) and a waist-to-height ratio of 0.66 indicating abdominal obesity with high cardiometabolic risk. Bioimpedance analysis confirmed an increased fat mass of 34% of total body weight, confirming obesity, and the visceral fat mass level of 19, almost twice the normal values, indicating a high risk of developing diabetes and, physiologically, contributing to the development of hypertension. The muscle mass ratio of 28.8% of total body weight is within normal limits. Repeated measurements confirmed stage 1 arterial hypertension in the patient. At the initial examination, his blood pressure was 147/96 mmHg. From a metabolic phenotypic classification standpoint, we classify the patient as having Metabolically Unhealthy Obesity (MUO). According to the EOSS obesity stage determination, the patient was previously evaluated as stage 1, with the presence of subclinical risk factors. However, the newly discovered arterial hypertension, the presence of comorbidity, moves the patient into stage 2, even without the presence of more severe psychological symptoms or functional limitations. We identified internal emotion, stress, as the trigger for his overeating. From the perspective of readiness for change, this patient experienced years of relapsing obesity, as he repeatedly failed to maintain his reduced body weight from previous attempts. However, the patient was aware that his behavior (stress eating, leading to weight gain) was problematic, typical of the contemplation phase, and after a long time, he contacted our clinic himself due to increased blood pressure values concurrent with weight gain. He sought professional help in his steps toward change because he could not achieve it on his own. Together, we created a treatment plan, and for hypertension treatment, we indicated a fixed combination of perindopril/amlodipine 10 mg/10 mg once daily. In addition to dietary and lifestyle measures, we have now added obesity pharmacotherapy - liraglutide with a gradual dose escalation to 3.0 mg subcutaneously daily, with a follow-up in 4 weeks. The patient came for a follow-up after 5 weeks, where we observed an excellent therapeutic effect (Figure 3c). In addition to a decrease in body weight by 7 kg (i.e., -6% from the original weight), there was also a reduction in waist circumference by 8 cm. The patient subjectively perceived the effects of liraglutide treatment even at the initial dose escalation of 0.6 mg, and the treatment allowed him to better plan meal times and reduce the size of each portion. Blood pressure values were optimized to 114/76 mmHg. Anticipating further weight loss and consequent reduction in blood pressure, we reduced the dose of the perindopril/amlodipine combination to 5 mg/5 mg once daily. The patient is motivated, adhering to the prescribed diet and exercise plan, and continues with further liraglutide treatment.
Table 1: Criteria defining the 4 basic phenotypes of obesity. Adapted from [6,7].
| MUNW (Metabolically unhealthy normal weight) | MHO (Metabolically healthy(pre)obesity) | MUO (Metabolically unhealthy(pre)obesity) | SO (Sarcopenic obesity | |
|---|---|---|---|---|
| Waist circumference | men < or ≥ 102 cm women < or ≥ 88 cm | men<102 cm women<88 cm | men≥102 cm women≥88 cm | men≥102 cm women≥88 cm |
| BMI | 18,5- 24,9 | BMI>25 | BMI>25 | BMI>25 |
| Visceral adipose tissue mass* | High | Low | High | High |
| Muscle mass* | - | High | - | Low |
| Metabolic abnormalities** | Present | Absent | Present | Present |
Conclusion
Despite obesity being defined as a chronic disease and easily diagnosable in patients, it is often overlooked and left untreated. With new pharmacological treatment options for obesity, such as liraglutide presented in the case studies, there is an opportunity in clinics to address obesity as a primary clinical concern. The presented case studies with different BMI values and various obesity phenotypes offer insight into obesity at different stages and forms of its development. They can serve as examples of early initiation of liraglutide treatment for obesity, which was initiated according to the new classification and monitored in the conditions of routine clinical practice. Shifting the indication for pharmacotherapy from BMI alone to the evaluation of other anthropometric and biochemical parameters, as well as functional and psychological status, comprehensively helps improve the health of patients with obesity.
References
- Busetto L, Dicker D, Frühbeck G, Halford JCG, Sbraccia P, et al. A new framework for the diagnosis, staging and management of obesity in adults. Nat Med. 2024. doi: 10.1038/s41591-024-03095-3.
- Sharma AM, Kushner RF. A proposed clinical staging system for obesity. Int J Obes (Lond). 2009; 33(3): 289-95.
- Swaleh R, McGuckin T, Myroniuk TW, Manca D, Lee K, et al. Using the Edmonton Obesity Staging System in the real world: a feasibility study based on cross-sectional data. CMAJ Open. 2021; 9(4): 1141-1148.
- Fábryová Ľ, Kissová V, Minárik P, Ukropcová B, Ukropec J, et al. Standard diagnostic and therapeutic guideline for complex management of overweight/obesity in adult age, 2nd revision (Štandardný diagnostický a terapeutický postup na komplexný manažment nadhmotnosti/obezity v dospelom veku 2. Revízia). Ministerstvo zdravotníctva Slovenskej republiky (mzsr.sk), Available at https://www.mzsr.sk/ Standardne-Postupy-V-Zdravotnictve.
- Sherf-Dagan S, Refaeli R, Buch A. Phenotyping of Obesity Treatment Candidates: A Narrative Review. Curr Obes Rep. 2024; 13(3): 564-573.
- Fábryová Ľ et al. Definition of Obesity in Clinical Obesitology (Definícia obezity v Klinická obezitológia), Facta Medica, Brno. 2023.
- Preda A, Carbone F, Tirandi A, Montecucco F, Liberale L. Obesity phenotypes and cardiovascular risk: From pathophysiology to clinical management. Rev Endocr Metab Disord. 2023; 24(5): 901-9196.
- Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012; 13(3): 275-86.
- Camacho-Barcia L, Lucas I, Miranda-Olivos R, Jiménez-Murcia S, et al. Applying psycho-behavioural phenotyping in obesity characterization. Rev Endocr Metab Disord. 2023; 24(5): 871-883.
- Málková I, Sucharda P, Málková H, Šlepecký M. Standad diagnostic and therapeutic guideline for psychological management of adults with overweight and obesity (Štandardný diagnostický a terapeutický postup pre psychologický manažment dospelých s nadváhou a obezitou), Ministerstvo zdravotníctva Slovenskej republiky (mzsr.sk), Available at https://www.mzsr.sk/ Standardne-Postupy-V-Zdravotnictve Summary of product characteristics Saxenda, www.ema.europa.eu.
- van Can J, Sloth B, Jensen CB, Flint A, Blaak EE, et al. Effects of the once-daily GLP-1 analog liraglutide on gastric emptying, glycemic parameters, appetite and energy metabolism in obese, non-diabetic adults. Int J Obes (Lond). 2014; 38(6): 784-93.
- Neeland IJ, Marso SP, Ayers CR, Lewis B, Oslica R, et al. Effects of liraglutide on visceral and ectopic fat in adults with overweight and obesity at high cardiovascular risk: a randomised, double-blind, placebo-controlled, clinical trial. Lancet Diabetes Endocrinol. 2021; 9(9): 595-605.
- Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JFet al. LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016; 375(4): 311-22.