
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Angiodysplasias by the meter: A rare case of an extensive gastrointestinal hemorrhage
Gualter Maria*; Marques R; Rouxinol M; Gonçalves I; Pinto-De-Sousa J
General Surgery, Local Health Unit of Trás-os-Montes and Alto Douro, Vila Real, Portugal.
*Corresponding Author : Gualter Maria General Surgery, Local Health Unit of Trás-os-Montes and Alto Douro, Vila Real, Portugal. Email: maria.gualter@hotmail.com
Received : Dec 11, 2024
Accepted : Jan 02, 2025
Published : Jan 09, 2025
Archived : www.jcimcr.org
Copyright : © Maria G (2025).
Abstract
Angiodysplasias, also known as vascular malformations, represent a heterogeneous group of vascular lesions characterized by abnormal, dilated blood vessels. They are often encountered in the gastrointestinal tract, particularly in the elderly population, and can lead to significant morbidity and mortality due to chronic blood loss or acute bleeding episodes. We report a case of a 76-year-old male who presented at the emergency department with gastrointestinal bleeding with unknown source. We describe clinical and intraoperative findings and the approach tailored to an atypical case of a not so rare anatomical anomaly.
Keywords: Angiodysplasia; Gastrointestinal haemorrhage; Thalidomide; Octreotide; .
Citation: Maria G, Marques R, Rouxinol M, Gonçalves I, Pinto-De-Sousa J. Angiodysplasias by the meter: A rare case of an extensive gastrointestinal haemorrhage. J Clin Images Med Case Rep. 2025; 6(1): 3416.
Introduction
Angiodysplasias (AD) are vascular abnormalities characterized by dilated, tortuous and usually small (<10 mm) blood vessels [1] that may occur throughout the Gastrointestinal (GI) tract. Since the first case was described in the literature, scholars have discussed about the precise cause of these lesions, leading to the use of different terms such as angioectasia, arteriovenous malformations and vascular ectasia. This etiology remains unclear, but they are often associated with aging and conditions that predispose to vascular abnormalities, as well as cardiovascular and pulmonary conditions, which could result in reduced blood flow to microvessels, leading to ischemic necrosis of anomalous vascular lesions [1]. The clinical presentation of bleeding angiodysplasias can range from asymptomatic to a life-threatening event, requiring emergent intervention. This bleeding can occur anywhere along the gastrointestinal tract length, but it is more commonly observed in the cecum, rectosigmoid area, the rest of colon, small intestine, and stomach, in descending order of frequency [2]. Angiodysplasias are usually diagnosed as an incidental finding during routine colonoscopy. The initial diagnostic modality depends on the characteristics of bleeding and suspicion for the location of the source, and usually follows the flowchart of any intestinal bleeding approach. Because AD is omnipresent throughout the GI tract, a combination of studies with endoscopy may be necessary. Upper GI endoscopy and colonoscopy are common initial diagnostic tools. Computed Tomography (CT) angiography and magnetic resonance angiography are also useful investigation tools, useful whenever conventional tools are not diagnostic regarding the bleeding origin [3]. Management of angiodysplasias largely depend on the clinical context in which it was diagnosed and depends on various factors including the severity of bleeding, location and size of the lesions, and the patient’s overall health status [1]. Treatment options may include endoscopic interventions, surgical resection or pharmacological approach. This case study emphasizes the available options for the treatment of this condition and on what assumptions clinicians could base their treatment decisions on.
Case report
A 76-year-old male patient presented to the Emergency Department with complaints of mental confusion, asthenia and pallor. He had a recent history of lacunar ischemic stroke in the left middle cerebral artery, with subsequent resolution of symptoms upon discharge. His medical history also included atrial fibrillation treated with edoxaban, valvular and hypertensive heart disease, chronic gastritis and colonic diverticulosis.


Initial evaluation by the Internal Medicine team revealed motor dysphasia, right homonymous hemianopsia, flattening of the right nasolabial fold, and ar right hemiparesis. He was normotensive, tachycardic, afebrile and had good peripheral oxygen saturations. A CT scan of the brain showed only ischemic sequelae, without acute lesions. An Electrocardiogram (ECG) revealed atrial fibrillation with rapid ventricular response. Blood tests showed a decrease in hemoglobin (7.1 g/dL), elevated transferrin (215 mg/dL), low transferrin saturation (15.6%), ferritin (52 pmol/L), urea (108 mg/dL), LDH (108 U/L) and an anti-Xa of 117. The patient denied gastrointestinal bleeding, palpitations, abdominal or chest pain. He was admitted to the Observation Room for further evaluation, during which he developed multiple episodes of melena. Two upper gastrointestinal endoscopies were performed, with the first being inconclusive due to solid gastric residues obstructing visualization, and the second revealing a small phlebectasia in the distal esophagus, with no abnormalities in the stomach or duodenum. A colonoscopy was attempted but limited to 30 cm from the anal margin due to abundant dark brown feces, with observed digested blood. A thoraco-abdomino-pelvic CT scan showed colonic diverticula without signs of acute diverticulitis or active bleeding. Despite remaining hemodynamically stable, the patient continued to experience bloody feces, progressing to hematochezia. On the fifth day of hospitalization, he remained without identified hemorrhagic focus. By this time, the patient had already received transfusion of ten units of blood. No platelets or plasma transfusion were performed in accordance to the Immunohemotherapy decision. After team discussion and considering that capsule endoscopy only provides diagnostic characterization and had a high probability of not being conclusive in a patient with active hemorrhage without transfusional benefit, and angiography was not available at the hospital, the patient was proposed for exploratory laparotomy.
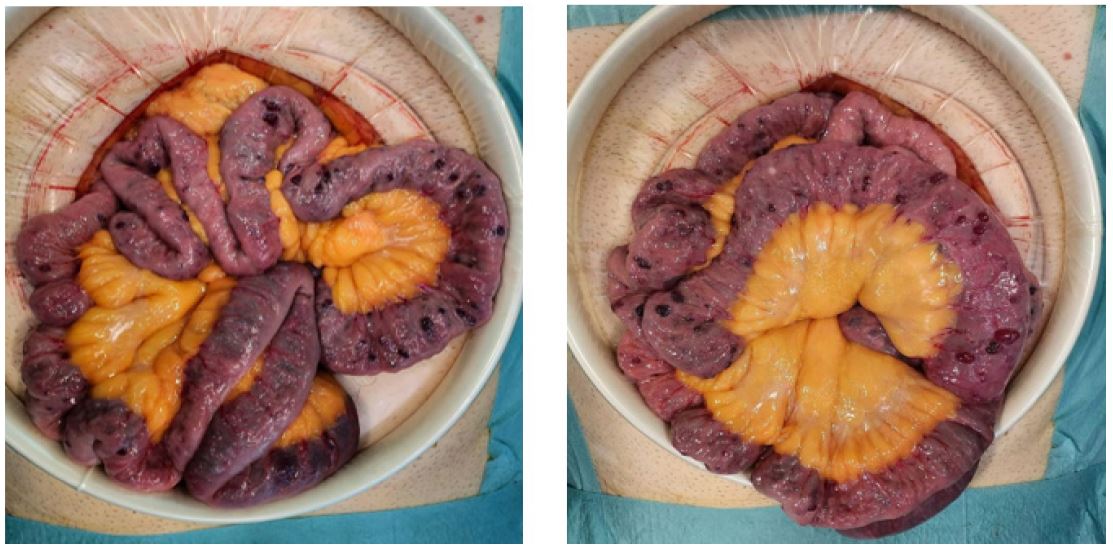
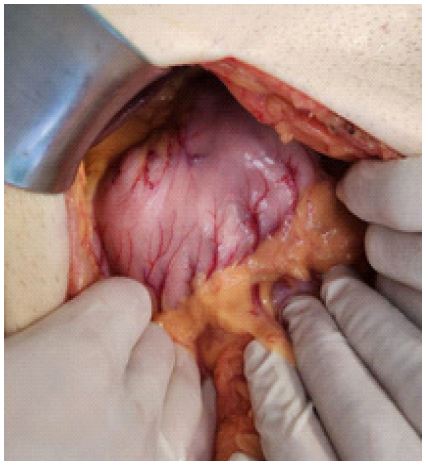
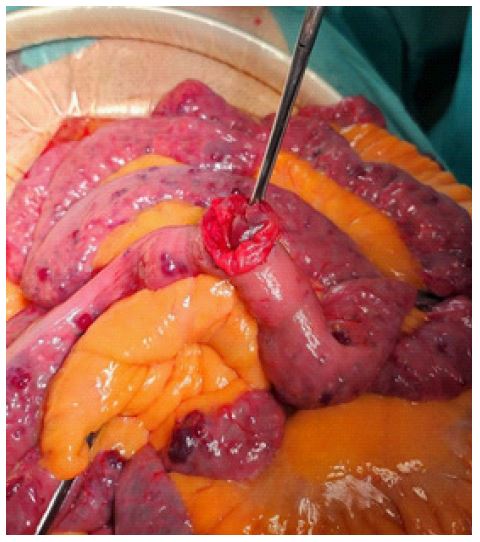
Intraoperatively, angiodysplasias were found throughout the small intestine (Figure 1a and 1b) and colon (Figure 2), as well as suspected vascular malformations in the stomach (Figure 3) and abdominal wall (Figure 4). Enterotomy of a small bowel loop was performed to check the direction of the bleeding, which was confirmed proximally and distally (Figure 5). Due to the extensive nature of the lesions and lack of surgical options, pharmacological treatment with octreotide was initiated after a review of the literature, with limited success expected. In the early postoperative period, the patient showed improved responsiveness, increased appetite, and controlled abdominal pain, with only one episode of melena. Treatment was switched to thalidomide for its oral availability, and the patient was discharged to a Continuing Care Unit on the seventy-third day of hospitalization (which was prolonged due to respiratory and cardiac complications), with stabilization of his hemorrhagic condition and no further bleeding episodes.
Discussion
Treatment is unnecessary for lesions discovered incidentally in patients experiencing non-bleeding symptoms or those who are asymptomatic. This is because the likelihood of future bleeding in these patient subgroups is low [4], and the majority of them continue to remain asymptomatic. The modalities for treating bleeding angiodysplasias, for those in need, include endoscopic therapies (argon plasma coagulation, mechanical clip placement, electrocoagulation and laser photoablation), angiography with embolization, surgical resection, and pharmacologic therapy [5].
Endoscopic therapy: An effective initial therapy, mostly used if angiodysplasia is present on endoscopy or colonoscopy. Different techniques can be used to treat angiodysplasia which is as follows.
Argon plasma coagulation ablation: It is the most commonly used intervention. This method usessynchronised delivery of electrical current and argon gas. The argon gas is ionised and allows transmission of the high-frequency current to the target lesion or tissuewithout direct contact.
Electrocoagulation: The first through-the-scope technique used to treat angiodysplasia. Uses bipolar or heater probe coagulation [1]. High risk of serious complications like bleeding or perforation particulary in the colon, where intestinal thin walls are present [6].
Endoscopic clips and band ligation: Successful mechanical methods to treat angiodysplasia. As a monotherapy or in combination with thermal ablation.
Photocoagulation (Laser): Photoablation of angiodysplasia with no serious complications reported in the last studies. High cost as limitation [1].
Angiography: Typically performed in patients experiencing active bleeding who have not responded to previously attempted treatments, those who are not suitable candidates for surgery, and to pinpoint bleeding sites as part of preoperative investigations before surgical resection.
Surgery: Progress in endoscopic and angiographic diagnostic and therapeutic capabilities has significantly decreased the necessity for surgical intervention in patients with bleeding AD. Surgical resection is now reserved for patients with heavy active bleeding requiring multiple blood unit transfusion when failed all other measures described above [1].
Pharmacological therapies: Treating AD with angiographic, endoscopic, and surgical methods may entail serious complications and may sometimes fail to prevent the recurrence of GI bleeding. This challenge arises because pinpointing the precise locations of all lesions, especially in the small bowel, can be difficult. Therefore, a safe and cost-effective pharmacological agent could serve as an appealing alternative. It may be suitable for patients with significant comorbidities, a high risk of complications from more invasive therapies, or those who do not respond to other treatment alternatives.
Hormone therapy: The most prevalent outcomes associated with treatment with estrogen with or without progesterone was the decrease in the number of bleeding episodes and need for transfusions.
Angiogenesis inhibitors: Thalidomide and bevacizumab effectiveness in the treatment of chronic bleeding from AD has been demonstrated in numerous published case reports [7]. A reduction in the number and size of AD has also been reported post-therapy.
Octreotide: The efficacy of the somatostatin analogue octreotide in mitigating bleeding from AD is attributed to various mechanisms, including the inhibition of angiogenesis by downregulating VEGF, increased vascular resistance, reduced splanchnic blood flow, and enhanced platelet aggregation [8]. While reports exist of endoscopic resolution of AD lesions following octreotide therapy, the extent of this effect has not been quantified [9]. Despite this, numerous case reports and case series have highlighted its significant benefits [10].
Conclusion
Vascular malformations should be considered as a cause of considerable gastrointestinal bleeding, as demonstrated in our patient. Overall, GI angiodysplasias represent a significant clinical challenge due to their potential to cause chronic occult bleeding or acute hemorrhage. Despite advancements in endoscopic and radiologic techniques, its diagnosis and treatment remain challenging. This proved to be an atypical case not only due to the extent of the ectasias, but also due to the excellent response to pharmacological therapy, in a case that was anticipated to have a poor prognosis. Further research is needed to elucidate the underlying mechanisms of angiodysplasias and to develop more effective and better-defined therapeutic strategies for this condition.
References
- Sami S, Al-Araji S, & Ragunath K. Review article: Gastrointestinal angiodysplasia-pathogenesis, diagnosis and management. Alimentary Pharmacology & Therapeutics. 2013; 39(1): 15-34. https://doi.org/10.1111/apt.12527.
- Boley SJ, DiBiase A, Brandt LJ, Sammartano RJ. Lower intestinal bleeding in the elderly. The American Journal of Surgery. 1979; 137(1): 57-64. https://doi.org/10.1016/0002-9610(79)90011-4.
- Richter JM, Hedberg SE, Athanasoulis CA, Schapiro RH. Angiodysplasia. Digestive Diseases and Sciences. 1984; 29(6): 481-485. https://doi.org/10.1007/bf01296266.
- Prevalence and natural history of colonic angiodysplasia among healthy asymptomatic people. 1995. https://pubmed.ncbi.nlm.nih.gov/7717311/.
- Jackson C, Strong RM. Gastrointestinal angiodysplasia. Gastrointestinal Endoscopy Clinics of North America. 2017; 27(1): 51-62. https://doi.org/10.1016/j.giec.2016.08.012.
- Aghighi M, Taherian M, Sharma A. 2023. Angiodysplasia. StatPearls-NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK549777/.
- Barkin JS, Ross BS. Medical therapy for chronic gastrointestinal bleeding of obscure origin. The American Journal of Gastroenterology. 1998; 93(8): 1250-1254. https://doi.org/10.1111/j.1572-0241.1998.404_i.x.
- Bauditz J, Lochs H, Voderholzer WA. Macroscopic appearance of intestinal angiodysplasias under antiangiogenic treatment with thalidomide. Endoscopy. 2006; 38(10): 1036-1039. https://doi.org/10.1055/s-2006-944829.
- Nardone G, Rocco A, Balzano T, & Budillon G. The efficacy of octreotide therapy in chronic bleeding due to vascular abnormalities of the gastrointestinal tract. Alimentary Pharmacology & Therapeutics. 1999; 13(11): 1429-1436. https://doi.org/10.1046/j.1365-2036.1999.00647.x.
- Brown CB, Subramanian V, Wilcox CM, Peter S. Somatostatin Analogues in the Treatment of Recurrent Bleeding from Gastrointestinal Vascular Malformations: An Overview and Systematic Review of Prospective Observational Studies. Digestive Diseases and Sciences. 2010; 55(8): 2129-2134. https://doi.org/10.1007/s10620-010-1193-6.