
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Superomedial subperiosteal orbital abscess in a child: A rare and severe complication of acute rhinosinusitis
Vera Miranda1*; Jorge Meira2; Roberto Estevão3 ; Nuno Álvaro Silva2; Miguel Campos Lopes1; Luciana Rodrigues1;
Tiago Soares Santos1
1ENT Department, Unidade Local de Saúde Entre o Douro e Vouga, Santa Maria da Feira, Portugal.
2Oftalmology Department, Unidade Local de Saúde São João, Porto, Portugal.
3ENT Department, Unidade Local de Saúde do Tâmega e Sousa, Penafiel, Portugal.
*Corresponding Author : Vera Miranda
ENT Department, Unidade Local de Saúde Entre o Douro e Vouga, Santa Maria da Feira, Portugal.
ORCID: https://orcid.org/0000-0002-8930-9383
Email: veracms@hotmail.com
Received : Dec 13, 2024
Accepted : Jan 03, 2025
Published : Jan 10, 2025
Archived : www.jcimcr.org
Copyright : © Miranda V (2025).
Abstract
Superomedial Subperiosteal Orbital Abscess (SSPOA) is a rare but severe complication of acute rhinosinusitis, particularly in pediatric patients. This case details a 10-year-old male presenting with progressive periorbital edema and proptosis following incomplete resolution of pre-septal cellulitis. High-resolution CT revealed a superomedial abscess associated with frontal sinus osteomyelitis. Treatment involved a multidisciplinary approach, combining empirical intravenous antibiotics and combined surgical approach with external drainage and endoscopic sinus surgery addressing the underlying pathology. The patient demonstrated immediate improvement postoperatively, with full recovery at long-term follow-up. This report emphasizes the importance of early diagnosis, multidisciplinary care, and tailored surgical interventions in managing rare orbital complications.
Keywords: Orbital cellulitis; Proptosis, Sinusitis; Orbital cellulitis; Frontal sinusitis; Pediatrics; Nasal surgery.
Citation: Miranda V, Meira J, Estevão R, Silva NA, Lopes MC, et al. Superomedial subperiosteal orbital abscess in a child: A rare and severe complication of acute rhinosinusitis. J Clin Images Med Case Rep. 2025; 6(1): 3418.
Introduction
Acute rhinosinusitis is a prevalent condition in pediatric populations, often self-limiting but with the potential for severe complications. Orbital involvement is among the most serious, occurring in approximately 5-10% of cases [1,2]. Anatomical proximity between the paranasal sinuses and orbit, combined with valveless venous drainage pathways, predisposes children to orbital complications, including pre-septal cellulitis, orbital cellulitis, and Subperiosteal Abscesses (SPOA) [3]. Chandler’s classification of orbital complications has provided a framework for understanding the progression of sinus-related orbital diseases, with subperiosteal abscesses representing an intermediate stage requiring timely intervention [2]. Superomedial Subperiosteal Orbital Abscesses (SSPOAs) are particularly rare, accounting for a small proportion of orbital infections but carrying significant risk due to their proximity to critical structures such as the optic nerve and cranial cavity [4,5]. Frontal sinus involvement is a frequent finding in SSPOAs and is often complicated by osteomyelitis of the orbital roof [6]. Clinical presentation can include progressive periorbital edema, restricted ocular motility, proptosis, and visual disturbances, requiring urgent diagnostic imaging. High-resolution Computed Tomography (CT) remains the gold standard for identifying abscesses, bony erosion, and associated complications [7,8].
Management of SSPOAs requires a combination of medical and surgical approaches. Empirical broad-spectrum antibiotics targeting common pathogens, such as Streptococcus pneumoniae, Haemophilus influenzae, and anaerobes, form the cornerstone of initial therapy [9]. Surgical intervention is often indicated in cases of significant abscess size (>1 cm), proptosis, or impaired ocular motility. Endoscopic sinus surgery has become the preferred approach for drainage of the affected sinuses [4], while external approaches are reserved for cases where endoscopic access is limited [4,10]. Multidisciplinary collaboration between otolaryngologists and ophthalmologists is essential to optimize outcomes and prevent complications [11]. This case exemplifies the successful integration of these principles in managing a pediatric patient with an SSPOA.
Case presentation
A previously healthy 10-year-old male presented in in emergency department with a 24-hour history of left superior periorbital edema, ocular pain, and fever. There were no associated symptoms such as nasal obstruction, cough, or headache. Clinical examination revealed moderate palpebral edema with mild erythema, preserved ocular motility, and no proptosis. A diagnosis of pre-septal cellulitis was made, and the patient was discharged with a eight-day course of oral amoxicillin-clavulanate (80 mg/kg/day). Despite partial improvement, the patient experienced significant worsening of left periorbital edema five days after completing the prescribed antibiotic course. Upon re-evaluation, he reported no fever, ocular pain, diplopia, nasal congestion or rhinorrhea. Ophthalmology and otolaryngology assessments were performed in the emergency department. Examination revealed limited left ocular mobility, especially in upward position, marked palpebral edema with erythema, mild temporal chemosis, and proptosis (Figure 1). Visual acuity was 8/10 bilaterally, and fundoscopic examination showed a well-defined optic disc without evidence of retinal abnormalities. Nasal endoscopy confirmed patency of the nasal cavity with no discharge or polyps.
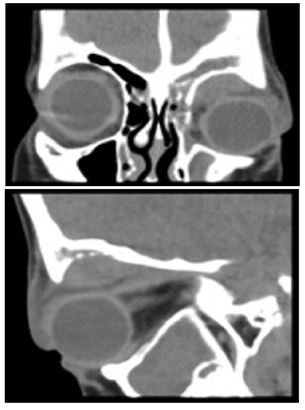
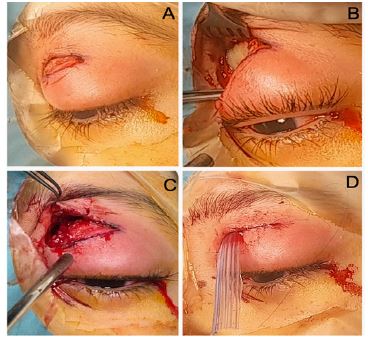
A complete blood count showed elevation of white blood cells (13.62×103/μL) with neutrophilia (61.7%), mild anemia (hemoglobin 11.1 g/dL), and thrombocytosis (574×103/μL). C-Reactive Protein (CRP) levels were normal (3.51 mg/L). The patient underwent a Computed Tomography (CT) that showed soft-tissue density opacification in the left frontal sinus, anterior ethmoid cells, and maxillary sinus, consistent with sinusitis (Figure 2). Erosive changes were noted in the inferior frontal sinus wall and orbital roof, with adjacent bone marrow hypodensities suggestive of osteomyelitis. A superomedial subperiosteal orbital abscess measuring 1.4×2.6×2.3 cm was identified, causing left ocular proptosis. Pre- and post-septal cellulitis with retrobulbar involvement was also evident, but the superior ophthalmic vein calibers were normal bilaterally. The patient was admitted with a diagnosis of left superomedial subperiosteal orbital abscess, a rare and severe complication of acute left rhinosinusitis. Intravenous therapy was initiated, including ceftriaxone (75 mg/kg/day), clindamycin (40 mg/kg/day), dexamethasone (0.3 mg/kg/day) and analgesics. Given the patient’s proptosis and impaired ocular mobility, urgent surgical intervention was planned and carried out by a multidisciplinary team involving ophthalmology and otorhinolaryngology specialists. Surgical management included external drainage of the abscess through a superior palpebral sulcus incision. The procedure involved careful dissection to the periosteum at the orbital roof, incision of the periorbita, and direct access to the abscess, allowing subsequent purulent material discharge. A drain was placed to ensure continuous drainage and prevent re-accumulation (Figure 3). Concurrently, endoscopic sinus surgery was performed through an anterior ethmoidectomy with drainage of the frontal sinus recess (Draf I), to address the underlying sinus disease. Both procedures were successfully completed without complications. The postoperative course was uneventful. The patient showed an immediate reduction in proptosis following surgery. Intravenous antibiotics and corticosteroids were continued for eight days. Intranasal corticosteroids (fluticasone furoate) and nasal saline irrigations were initiated to promote sinus healing. The drain was removed on the fifth postoperative day. After a total of eight days of hospitalization, the patient was discharged with instructions to continue oral antibiotics and intranasal medication. Significant clinical improvement was noted at discharge, with complete resolution of palpebral edema and erythema, preserved ocular motility, and no residual proptosis. At a follow-up examination two weeks later, the healing process was confirmed to be normal, and the patient was asymptomatic. Four months postoperatively, the patient had achieved full recovery with no residual symptoms or functional deficits.
This case illustrates the challenges and key considerations in diagnosing and managing SSPOA a rare but severe complication of acute rhinosinusitis. The patient presented with progressive periorbital edema and proptosis, consistent with findings in similar cases described in the literature [3]. While the initial presentation was suggestive of pre-septal cellulitis, the subsequent worsening of symptoms despite appropriate antibiotic therapy highlighted the importance of reassessment and imaging in cases of treatment failure. CT scan played a pivotal role in confirming the diagnosis, revealing bony erosions and a large superomedial orbital abscess associated with frontal sinus osteomyelitis. Dankbaar et al. emphasize the value of CT in delineating abscess size, location, and associated complications such as intracranial spread, which are critical for surgical planning [12]. The choice of surgical approach in this case was guided by the abscess’s size and location. The combination of external drainage via a superior palpebral sulcus incision and endoscopic sinus surgery allowed for effective evacuation of the abscess and comprehensive management of the underlying sinus disease. This dual approach aligns with recommendations by Ketenci et al. who advocate for tailored surgical strategies based on the anatomical complexity of SSPOAs [10].
Empirical antibiotic therapy, initiated prior to surgery, targeted common pathogens involved in orbital complications of rhinosinusitis. Brook et al. highlight the importance of covering Streptococcus species, Staphylococcus aureus, and anaerobes, which are frequently implicated in such infections [9]. The addition of corticosteroids, though debated, contributed to the rapid reduction in orbital inflammation and proptosis, consistent with findings reported by Gavriel et al. [11]. Multidisciplinary collaboration was a cornerstone of successful management in this case. The involvement of both otolaryngology and ophthalmology teams ensured comprehensive care, addressing both the orbital and sinonasal components of the disease. Yang et al. emphasize that such coordinated care is essential in complex cases involving orbital complications of rhinosinusitis [13]. Long-term follow-up demonstrated complete resolution of symptoms without functional or cosmetic sequelae. This favorable outcome underscores the importance of early diagnosis, prompt intervention, and a multidisciplinary approach in managing SSPOAs. The principles applied in this case are supported by multiple studies and serve as a model for managing similar presentations in pediatric patients.

Conclusion
This case underscores the critical importance of early diagnosis and timely intervention in managing SSPOA. Multidisciplinary collaboration between otolaryngology and ophthalmology teams is essential for achieving optimal outcomes. The external surgical approach performed by orbital specialists was instrumental in this case, ensuring effective drainage and resolution of the abscess while preserving the patient’s vision and functionality. These findings highlight the need for a tailored, multidisciplinary approach in managing rare and complex orbital complications of rhinosinusitis.
Conflicts of interest: The authors declare no conflicts of interest.
ORCID IDs of all authors
Roberto Estevão: https://orcid.org/0000-0002-5415-6858
Nuno Álvaro Silva: https://orcid.org/0000-0001-8918-8027
Miguel Campos Lopes: https://orcid.org/0000-0002-7112-3580
Luciana Rodrigues: https://orcid.org/0000-0002-2901-4129
Tiago Soares Santos: https://orcid.org/0000-0003-2706-7531
References
- Wald ER, Guerra N, Byers C. Upper respiratory tract infections in young children: duration of and frequency of complications. Pediatrics. 1991; 87(2): 129-133.
- Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970; 80(9): 1414-1428. doi:10.1288/00005537-197009000-00007.
- Chrysovitsiotis G, Kollia P, Kyrodimos E, Chrysovergis A. Superiorly based subperiosteal orbital abscess: an uncommon presentation. BMJ Case Rep. 2021; 14(2): 239861. doi:10.1136/bcr-2020-239861.
- Wong S, Levi J. Management of pediatric orbital cellulitis: A systematic review. International Journal of Pediatric Otorhinolaryngology. 2018; 110(1). DOI:10.1016/j.ijporl.2018.05.006.
- Bedwell J, Bauman NM. Management of pediatric orbital cellulitis and abscess. Curr Opin Otolaryngol Head Neck Surg. 2011; 19(6): 467-473. doi:10.1097/MOO.0b013e32834cd54a.
- Liao JC, Harris GJ. Subperiosteal abscess of the orbit: Evolving pathogens and the therapeutic protocol. Ophthalmology. 2015; 122(3): 639-647. doi:10.1016/j.ophtha.2014.09.009.
- Chaudhry IA, Al-Rashed W, Arat YO. The hot orbit: Orbital cellulitis. Middle East Afr J Ophthalmol. 2012; 19(1): 34-42. doi:10.4103/0974-9233.92114.
- Leung AK, Hon KL, Chu WC. Acute bacterial sinusitis in children: an updated review. Drugs Context. 2020; 9: 2020-9-3. doi:10.7573/dic.2020-9-3.
- Brook I. Microbiology and antimicrobial treatment of orbital and intracranial complications of sinusitis in children and their management. Int J Pediatr Otorhinolaryngol. 2009; 73(9): 1183-1186. doi:10.1016/j.ijporl.2009.01.020.
- Ketenci I, Unlü Y, Vural A, Doğan H, Sahin MI, Tuncer E. Approaches to subperiosteal orbital abscesses. Eur Arch Otorhinolaryngol. 2013; 270(4): 1317-1327. doi:10.1007/s00405-012-2198-x.
- Gavriel H, Jabrin B, Eviatar E. Management of superior subperiosteal orbital abscess. Eur Arch Otorhinolaryngol. 2016; 273(1): 145-150. doi:10.1007/s00405-015-3557-1.
- Dankbaar JW, van Bemmel AJ, Pameijer FA. Imaging findings of the orbital and intracranial complications of acute bacterial rhinosinusitis. Insights Imaging. 2015; 6(5): 509-518. doi:10.1007/s13244-015-0424-y.
- Yang M, Quah BL, Seah LL, Looi A. Orbital cellulitis in children-medical treatment versus surgical management. Orbit. 2009; 28(2-3): 124-136. doi:10.1080/01676830902765891.