
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Cavitary sarcoidosis complicated by aspergilloma
Mariana Nunes*; Elisabete Cerqueira; Beatriz Riquito; Mariana Certal; Olivia Cardoso
Internal Medicine, Chaves Hospital, Unidade Local de Saúde de Trás-os-Montes e Alto Douro, Portugal.
*Corresponding Author : Mariana Nunes
Internal Medicine, Chaves Hospital, Unidade Local de Saúde de Trás-os-Montes e Alto Douro, Portugal.
Tel: +351917884250;
Email: marianasilva.17@hotmail.com
Received : Dec 18, 2024
Accepted : Jan 06, 2025
Published : Jan 13, 2025
Archived : www.jcimcr.org
Copyright : © Nunes M (2025).
Abstract
Pulmonary sarcoidosis is a granulomatous disorder that can lead to chronic and progressive lung damage. Cavitation is an uncommon complication, but when it occurs, it may create an environment favorable to secondary infections, including aspergilloma formation. Such complications significantly increase the risk of life-threatening events like massive hemoptysis. A 59-year-old retired construction worker with a 10-year history of pulmonary sarcoidosis. Multiple therapeutic attempts were made, including corticosteroids, which yielded no improvement, and methotrexate, discontinued due to intolerance. Over time, his disease progressed, necessitating long-term oxygen therapy, which the patient did not consistently follow. Five years after his initial diagnosis, a chest CT scan revealed a cavitary lesion in the right upper lobe consistent with aspergilloma. Although itraconazole therapy was indicated, the patient failed to adhere to the prescribed regimen. Two years later, he presented to the emergency department with massive hemoptysis and ultimately succumbed to this complication.
Keywords: Pulmonary sarcoidosis; Aspergilloma; Cavitary lung lesion; Antifungal therapy; Massive hemoptysis.
Citation: Nunes M, Cerqueira E, Riquito B, Certal M, Cardoso O. Cavitary sarcoidosis complicated by aspergilloma. J Clin Images Med Case Rep. 2025; 6(1): 3420.
Introduction
Aspergilloma, a collection of Aspergillus hyphae and debris within pre-existing lung cavities, can occur as an uncommon but serious complication in patients with advanced pulmonary sarcoidosis. Although sarcoidosis primarily affects the lungs, it only occasionally leads to cavitary lesions. When cavities form, they provide a favorable environment for fungal colonization by Aspergillus. Patients may present with few or nonspecific symptoms, but hemoptysis-ranging from mild to life-threatening-is a significant concern. Diagnosis typically involves imaging (particularly high-resolution CT) and, eventually, microbiological and serological tests. Treatment options include antifungal therapy with oral azoles, although these may have limited efficacy in penetrating the fungal ball. Severe cases might require surgical intervention or bronchial artery embolization. Early recognition, thorough evaluation, and a multidisciplinary approach are critical for preventing severe complications and improving patient outcomes.
Case description
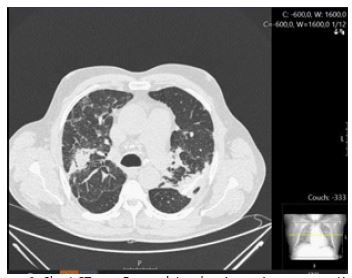
A 59-year-old retired construction worker had been diagnosed with pulmonary sarcoidosis 10 years earlier (Figure 1). He underwent several courses of treatment, including corticosteroids, which proved ineffective, and later methotrexate, which was discontinued due to intolerance. His condition worsened, eventually requiring supplemental oxygen therapy, which he did not use regularly. Five years after the initial diagnosis, a chest CT scan (Figure 2) revealed a cavitary lesion in the right upper lobe suggestive of aspergilloma. Although itraconazole therapy was indicated, he was noncompliant. Two years later, he presented to the emergency department with massive haemoptysis, which ultimately caused his death.

Conclusion
In summary, although relatively uncommon, the development of aspergilloma in a sarcoidosis- related lung cavity represents a severe and potentially life-threatening complication. This case underscores the critical importance of early recognition and treatment of aspergilloma in advanced pulmonary sarcoidosis. Adherence to antifungal therapy and close multidisciplinary follow-up are paramount to preventing catastrophic outcomes. The patient’s nonadherence to therapeutic measures and the advanced stage of his disease contributed to a fatal outcome, highlighting the need for patient education, support, and rigorous management strategies.
References
- Denning DW. Chronic pulmonary aspergillosis. Eur Respir J. 2003; 21(6): 865-868.
- Palomar-Lever A, Pavón-Vergés M, Bazaldúa-Penalba A, Carrillo-Sánchez JD, Chavira-Pérez Hemoptysis due to Aspergillus cavitation in sarcoidosis: A case report and review of the literature. Sarcoidosis Vasc Diffuse Lung Dis. 2019; 36(3): 233-236.
- Kahl FA, Albers GM, Williams DE, Aye RW. Aspergilloma in a sarcoidosis cavity: Diagnosis and treatment. Can Med Assoc J. 1971; 104(12): 1167-1170.
- Patterson KC, Strek ME. Pulmonary fibrosis in sarcoidosis: A review. Respirology. 2014; 19(7): 795-803.