
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Takotsubo cardiomyopathy and pregnancy: A case report
Cecilia Galli1; Giulia D’ovidio1*; Federica Del Prete1; Chiara Mandosi1; Gianluca Agnes2; Fabio Ferrante2ss; Maria Grazia Piccioni1
1Department of Maternal, Infantile and Urological Sciences, University of Rome La Sapienza, Viale del Policlinico 155, 00161 Rome, Italy.
2Department of Cardiovascular/Respiratory Diseases, Nephrology, Anesthesiology, and Geriatric Sciences, Policlinico Umberto I, Sapienza University of Rome, Rome, Italy.
*Corresponding Author : Giulia D’Ovidio
Department of Maternal, Infantile and Urological Sciences, University of Rome La Sapienza, Viale del Policlinico 155, 00161 Rome, Italy.
Email: g.dovidio@uniroma1.it
Received : Dec 11, 2024
Accepted : Jan 07, 2025
Published : Jan 14, 2025
Archived : www.jcimcr.org
Copyright : © D’ovidio G (2025).
Abstract
Background: Takotsubo Syndrome (TTS) is a particular clinical condition that can mimic an acute myocardial infarction. Myocardial injury may be due to a pathological effect of catecholamines caused by emotional stress or to as yet unidentified genetic mutations that predispose to this type of alterations. Takotsubo syndrome is a fairly rare event: the prevalence of TTS in the general population is approximately 2% in patients with presumed acute coronary disease.
Methods: We described the case of a 38-year-old woman, pregnant at 24 weeks, followed at the Policlinico Umberto I in Rome, in whom Takotsubo cardiomyopathy was diagnosed, focusing on diagnosis and treatment.
Results: Although several cases of Takotsubo cardiomyopathy arising in the peripartum or postpartum have been reported in the literature, the diagnostic and therapeutic process is complex and requires a specific case-by-case study. A multidisciplinary team work is necessary throughout the pregnancy, to decide the correct therapeutic procedure and the time of delivery and to prepare the cesarean sectionin a timely manner if necessary.
Conclusion: A timely diagnosis, with continuous monitoring of fetal and maternal well-being, is essential for a good prognosis.
Keywords: Takotsubo Syndrome (TTS); Pregnancy; Multidisciplinary management.
Citation: Galli C, D’ovidio G, Prete FD, Mandosi C, Agnes G, et al. Takotsubo cardiomyopathy and pregnancy: A case report. J Clin Images Med Case Rep. 2025; 6(1): 3423.
Introduction
Takotsubo Syndrome (TTS), also known as broken heart syndrome, is a particular clinical condition capable of mimicking an acute myocardial infarction. It is manifested by retrosternal pain, ECG changes, increased myocardial necrosis indices. Its main feature is the absence of coronary vascular lesions such as to justify this clinical picture [1-3]. There are several theories on the cause of this condition: the first is that the myocardial lesion is due to a pathological effect of the catecholamines due to emotional stress, the second is that there are genetic mutations not yet identified capable of predisposing to this type of alterations [4]. Several variants of Takotsubo syndrome are described in the literature: Classic scheme: 80% of patients. Middle ventricular pattern: Hypokinesia of the left middle ventricle and hypercontractile apical and basal segments (15%). Inverted (inverse) pattern: Hypokinesia or akinesia of the basal and middle ventricular segments with preserved contractility or hypercontractility of the apical segments. Present in 2-5% of patients. Focal type: Hypokinesia or akinesia of an isolated segment; usually an anterolateral segment. Present in up to 1.5% of patients.
Atypical patterns with right ventricular involvement: apical tip sparing variant, apical biventricular dysfunction, isolated right ventricular involvement, and global type [5].
The takotsubo syndrome is a fairly rare event: the prevalence of TTS in the general population is approximately 2% in patients with supposed acute coronary artery disease; usually over 90% of TTS patients are post-menopausal women [6], however, there are no data in the literature capable of quantifying the prevalence of this condition in pregnancy. Although generally considered a benign condition, it can be burdened with serious complications such as cardiogenic shock,ventricular rupture,or malignant arrhythmias [7]. The symptoms most frequently associated with are chest pain (67%) and dyspnoea (17%) [8]. It is also often found in some psychiatric conditions such as depression or anxiety. In pregnancy there is a strong association between Takotsubo syndrome and postpartum depression [9]. Most cases of TTS in pregnancy are described in the peripartum period regardless of how this occurs [10-12] which makes it difficult to differentiate TTS from other peripartum cardiomyopathy.
Case report
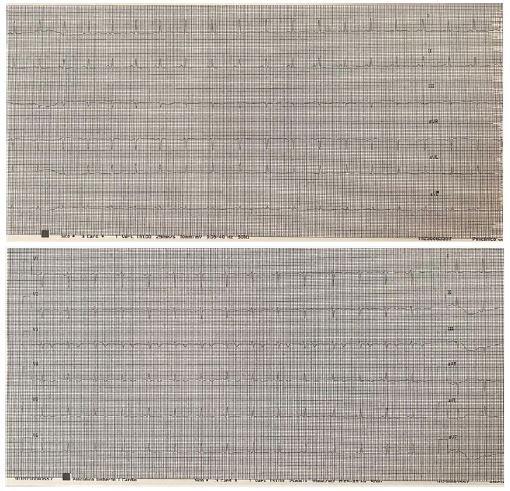
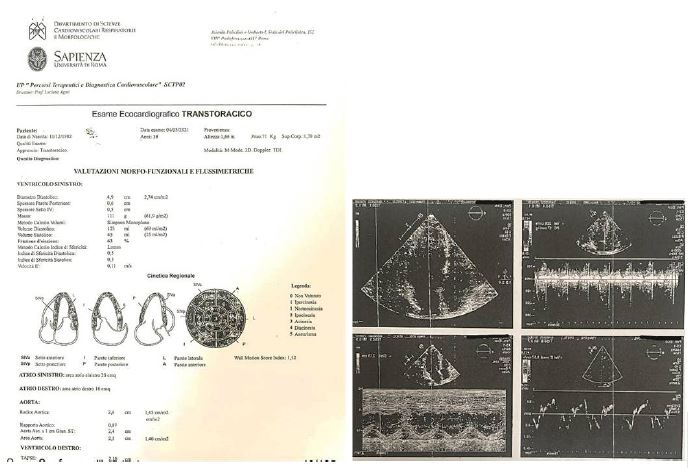
A 38-year-old woman, 24 weeks pregnant, arrives at the General Emergency Department of the Policlinico Umberto I in Rome, transferred from another hospital, for suspected NSTEMI (Non-ST-Elevation Myocardial Infarction) associated with chest pain that varies with breathing and movements, radiating to the arms and neck. In history, the patient had a family history of diabetes mellitus and chronic hypertension, but she denied notable disease or previous surgery. In her obstetric history she reported a previous spontaneous delivery at term. The course of the previous pregnancy was entirely physiological. In the emergency department, an ECG was performed showing a heart rate of 100 bpm, axis balanced, with inverted T waves in leads V1 to V4 and a transthoracic echocardiogram showing mildly depressed global systolic performance (EF 45%), with hypokinesia of the apex and hyperkinesis of the basal segments. Absence of pericardial effusion. The patient was hemodynamically stable. First biochemical examinations showed the following results: creatine kinase 504 UI/L, creatine kinase-MB 33.3 ng/ml, myoglobin 22, LDH 330, high sensitivity troponin T 0.970 mcg/L, pro-Brain Natriuretic Peptide (BNP) 450 pg/ml. An obstetric consultation is performed in which an OFFICE ultrasound shows a live and viable fetus in a longitudinal situation with preserved fetal well-being, the presence of an amniochorial detachment at the level of the lower pole has been reported. The patient is admitted to the Cardiology department of this hospital, upon admission she was alert and oriented with normal vital parameters and a stable ECG compared to the one performed in the Emergency Department. During hospitalization, a new echocardiographic evaluation was also performed which showed left ventricles of normal size with normal systolic performance (EF 63%) and apex akinesia; right sections of dimensions within the limits with normal systolic performance of the right ventricle, absence of pericardial effusion. The patient is monitored daily from a haemodynamic and obstetric point of view and conserconservative medical therapy is decided (class II indication, LOE A) on the basis of her haemodynamic stability and considering the high teratogenic risk from ionizing radiation used for a possible procedure coronary angiography, subject to obtaining informed consent from the patient. Medical therapy consisted of cardioaspirin 100 mg and enoxaparin 4000 IU. The patient was discharged in good general condition and absence of angor after ten days of hospitalization with home therapy (Enoxaparin 4000 I.U.).
The patient was hospitalized again at 37 weeks and 4 days in the Delivery Room of the Umberto I Polyclinic in Rome to perform an elective cesarean with extraction of a single live and viable male fetus weighing 3810 g, Apgar 9/10, pH 7.29. Blood pressure and other vital signs were normal throughout the puerperal period. She is discharged from the delivery room with home therapy (Enoxaparin 4000 IU) for a further 15 days post-CT.
Discussion and conclusion
Although several cases of Takotsubo cardiomyopathy arising in the peripartum or postpartum are presented in the literature, the diagnostic and therapeutic pathway is complex and requires a specific case-by-case study. The etiology of the disease remains unknown in many cases. Although our case presented a favorable prognosis, several aspects of this form of cardiomyopathy must be taken into consideration. Sudden death is probably not so rare in the onset of TTS: ventricular fibrillation may occur on the basis of severe left ventricular impairment, but arrhythmia related to QTc interval prolongation during the early period may also be of disease. The recovery of cardiac function must therefore be rapid, for the prognosis to be good [13]. Therapy with adrenaline (or other amines) under emergency conditions may play a role in the clinical setting [14]. Diagnostic evaluation of TTS includes an Electrocardiogram (ECG), cardiac biomarkers, echocardiography of the left heart. ECG pattern may vary from ST segment elevation in the anterior and precordial leads, not explained by a single coronary artery distribution, to ST-segment depression (10% of cases). Usually after 12-24 h the ECG pattern changes and shows symmetric T wave inversion and QTc prolongation [14,15]. Most patients have abnormal cardiac troponin values associated with normal creatinine kinase. Natriuretic peptides (Brain Natriuretic Peptide (BNP) and pro-BNP) may be elevated indicating ventricular involvement, to a lesser extent than seen in acute myocarditis and this allows for differential diagnosis [16]. Typical findings of transthoracic echocardiography include a large area of regional akinesia of left ventricular wall motion extending beyond the territory of a single coronary [17]. There is apical swelling of the left ventricle with normal basal contractility. Left ventricular ejection fraction is often reduced by 20 to 49% [18]. Additionally, there may be mitral regurgitation with or without systolic movement of the anterior leaflet [19]. Diagnosis is based on the Mayo Clinic diagnostic criteria [20]. This includes the presence of transient akinesia, hypokinesia, or dyskinesia of the left ventricle with or without apical involvement; This regional ventricular wall motion abnormality extends beyond a single territory of epicardial vascular perfusion. Furthermore, there is no obstructive coronary artery disease or angiographic evidence of acute plaque rupture. From an obstetric point of view, correct management involves an assessment of fetal well-being on a daily basis until normal maternal cardiovascular function is restored. Possible growth limitations, lack of perception of fetal movements by the mother, oligoamnios are to be considered alarm factors and require adequate planning of the birth. Resolution of physical or emotional stress usually results in rapid resolution of symptoms, although some patients may develop acute complications such as acute heart failure and cardiogenic shock requiring admission to coronary care units and the need for invasive techniques such as intra-aortic and cardiopulmonary [21]. The decision on the timing and mode of delivery should be guided by obstetric reasons. It should involve a multidisciplinary team of cardiologists, obstetricians, neonatologists and psychologists. From our experience, in the suspected diagnosis of Takotsubo syndrome in pregnancy, we have suggested transferring the patient to a tertiary care center where she can be followed up both from a cardiovascular and an obstetric point of view. Timely diagnosis, with continuous monitoring of fetal and maternal well-being, is essential for a good prognosis. A multidisciplinary work is necessary throughout the pregnancy, to decide the correct therapeutic procedure and the timing of the birth and promptly prepare the surgery.
References
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015; 373(10): 929-38.
- Minatoguchi M, Itakura A, Takagi E, Nishibayashi M, Kikuchi M, et al. Takotsubo cardiomyopathy after cesarean: a case report and published work review of pregnancy-related cases. J Obstet Gynaecol Res. 2014; 40(6): 1534-9.
- Salmoirago-Blotcher E, Dunsiger S, Swales HH, Aurigemma GP, Ockene I, et al. Reproductive history of women with Takotsubo cardiomyopathy. Am J Cardiol. 2016; 118(12): 1922-8.
- Dennis AT, Castro JM. Echocardiographic differences between preeclampsia and peripartum cardiomyopathy. Int J Obstet Anesth. 2014; 23: 260-6.
- Citro R, Giudice R, Mirra M, Bottiglieri G, Bossone E, et al. Tako-tsubo syndrome soon after caesarean delivery: two case reports. Int J Cardiol. 2012; 161: 48-9.
- Kristian Thygesen, Joseph S Alpert, Allan S Jaffe, Bernard R Chaitman, Jeroen J Bax, et al. Fourth universal definition of myocardial infarction. European Heart Journal. 2018; 40(3): 237-269. https://doi.org/10.1093/eurheartj/ehy462.
- Lyon AR, Bossone E, Schneider B, SechtemU, Citro R, et al. CurrentstateofknowledgeonTakotsubosyndrome:A PositionStatement fromtheTaskforceonTakotsuboSyndromeof theHeart Failure Associationof theEuropeanSocietyofCardiology.Eur JHeartFail. 2016; 18: 8-27.
- Ueyama T. Emotional stress-induced Tako-tsubo cardiomyopathy: animal model and molecular mechanism. Ann N Y Acad Sci. 2004; 1018: 437-444.
- Masiarek K, Grabowicz W, Makowski M, Frynas K, Szyłło N, et al. Zespół tako-tsubo - forma ostrego zespołu wieńcowego czy całkiem odmienna jednostka chorobowa? Opis przypadku [Tako-tsubo syndrome - a form of acute coronary syndrome or completely different clinical entity - a case report]. Kardiol Pol. 2010; 68(1): 66-71. Polish. PMID: 20131190.
- Virani SS, Khan AN, Mendoza CE, Ferreira AC, de Marchena E. Takotsubo cardiomyopathy, or broken-heart syndrome. Tex Heart Inst J. 2007; 34(1): 76-9.
- Ruiz S, Martinez-Marin M, Luque P, Nassar N, Oros D. Takotsubo cardiomyopathy after cesarean section: A case report and literature review. J Obstet Gynaecol Res. 2017; 43(2): 392-6.
- Suzuki T, Nemoto C, Ikegami Y, Yokokawa T, Tsukada Y, et al. Development of takotsubo cardiomyopathy with severe pulmonary edema before a cesarean section. J Anesth. 2014; 28(1): 121-4.
- D’Amato N, Colonna P, Brindicci P, Campagna MG, Petrillo C, et al. Tako-Tsubo syndrome in a pregnant woman. Eur J Echocardiogr. 2008; 9(5): 700-3. doi: 10.1093/ejechocard/jen135.
- TemplinC, Ghadri JR, Diekmann J, Napp LC, BataiosuDR, et al. Lu¨scher Clinical featuresandoutcomesof takotsubo(stress)cardiomyopathy.NEngl JMed. 2015; 373: 929-938.
- MedeirosK O, Connor MJ, Baicu CF, Fitzgibbons TP, Shaw P, et al. Systolic and diastolic mechanics in stress cardiomyopathy. Circulation. 2014; 129: 1659-1667. Rozema T, Klein LR. Takotsubo cardiomyopathy: Acase report and literature review. Cardiol Young. 2016; 26(2):406-9.
- Gupta S, Gupta MM. Takotsubo syndrome. Indian Heart J. 2018; 70(1): 165-74.
- Roshanzamir S, Showkathali R. Takotsubo cardiomyopathy a short review. Curr Cardiol Rev. 2013; 9(3): 191-6.
- Yalta K, Yilmaztepe M, Zorkun C. Left ventricular dysfunction in the setting of Takotsubo cardiomyopathy: A review of clinical patterns and practical implications. Card Fail Rev. 2018; 4(1): 14-20.
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015; 373(10): 929-38.
- De Backer O, Debonnaire P, Gevaert S, Missault L, Gheeraert P, et al. Prevalence, associated factors and management implications of left ventricular outflow tract obstruction in takotsubo cardiomyopathy: A twoyear, two-center experience. BMC Cardiovasc Disord. 2014; 14: 147.
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, et al. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006; 27: 1523-1529. doi: 10.1093/eurheartj/ehl032.