
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Diagnosis of a mitral valve blood cyst in a 16-year-old asymptomatic male athlete: A case report
Perlepe Kalliopi1*; Rozos Panagiotis1; Karanasios Evangelos2; Nyktari Evangelia1; Thomas Vrachliotis1; Soultana Kourtidou1
1Cardiac MRI Unit, Onassis Cardiac Surgery Center, Athens, Greece.
2Cardiology Department, “Aghia Sophia” Children’s Hospital, Athens, Greece.
*Corresponding Author : Perlepe Kalliopi
Cardiac MRI Unit, Onassis Cardiac Surgery Center, Athens, Greece.
Tel: 00306974298223;
Email: perlepe.popy@gmail.com
Received : Dec 18, 2024
Accepted : Jan 08, 2025
Published : Jan 15, 2025
Archived : www.jcimcr.org
Copyright : © Kalliopi P (2025).
Abstract
Congenital intracardiac blood cysts are rare benign malformations that tend to regress spontaneously during infancy. As such, their reported incidence among older children and adults is extremely low. Although mainly asymptomatic, they are commonly located along the closing lines of the heart valves causing concern regarding their potential for valve dysfunction and obstructive or thromboembolic phenomena. Echocardiography is adequate for the initial identification of the lesion and functional assessment of the valve; however, Cardiac Magnetic Resonance Imaging (CMR) is pivotal in the differential diagnosis from other cardiac masses. We present a case of a 16-year-old asymptomatic male athlete referred for CMR due to a mitral valve mass that was incidentally found on echocardiography. Based on CMR features a diagnosis of a blood cyst was made, and due to the lack of complications, a conservative approach was decided. The patient remained stable during the follow-up period.
Keywords: Blood cyst; Mitral valve; Cardiac magnetic resonance; Cardiac tumors; Case report.
Citation: Kalliopi P, Panagiotis R, Evangelos K, Evangelia N, Vrachliotis T, et al. Diagnosis of a mitral valve blood cyst in a 16-year-old asymptomatic male athlete: A case report. J Clin Images Med Case Rep. 2025; 6(1): 3424.
Background
Intracardiac blood cysts seem to be a common finding in autopsies of fetuses and infants below 2 months of age, but they tend to resolve spontaneously being a rare finding in older infants, children, and adults [1,2]. Literature is sparse, particularly among pediatric patients [3-9]. Considering the rarity of such finding, multimodality imaging evaluation is often required to differentiate the mass and alleviate the stress related to alternative tumors. We report the case of a 16-year-old asymptomatic male athlete, and his comprehensive Cardiac Magnetic Resonance (CMR) imaging approach to establish his diagnosis of a mitral valve blood cyst.
Case report
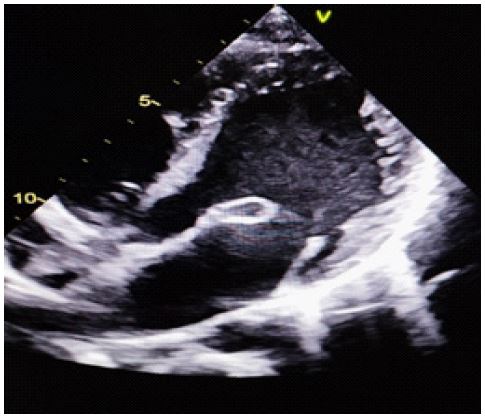
A 16-year-old boy, elite athlete, was referred to our CMR department following the detection of a mitral valve lesion during a routine cardiology visit for sports participation screening. Patient revealed no past medical or surgical history. Interestingly, his mother reported some mitral valve abnormality as well. Review of systems was negative for constitutional symptoms. Vital signs, physical examination and baseline electrocardiogram were normal. Transthoracic echocardiography was unremarkable except for a rather round, cystic – like, mobile mass located at the tip of the anterior mitral leaflet, causing no obstruction or regurgitation (Figure 1). A non-sedated CMR with contrast (Gadavist 0.15 ml/kg IV) at a 1.5T Siemens Sola scanner, was obtained for tissue characterization and further differentiation of the mass. Cine images showed a small (16x12 mm) ovoid, well-circumscribed mobile heterogenous lesion with smooth borders, attached to the ventricular side of the tip of the anterior mitral valve leaflet. There was no left ventricular outflow obstruction. The lesion was Isointense to the myocardium on balanced steady state free precession (b-SSFP) cine images (Figure 2, Panels A-B).
Isointense on breath-hold T1 weighted Turbo Spin Echo (TSE) with double inversion pulse sequences (Figure 2, Panel C) and remained isointense when a fat saturation pulse was added, confirming that its nature was not lipomatous.
Hyperintense with diffusely increased signal on T2 weighted TSE double inversion sequences with and without fat suppression (Figure 2, Panels D-E) suggestive of its cystic nature.
Following contrast administration, the lesion showed:
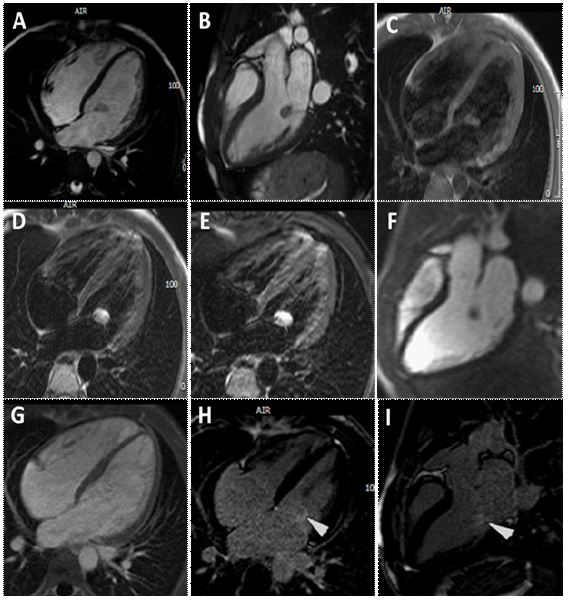
No gadolinium absorption on first pass perfusion (Figure 2, Panel F).
Absence of thrombus characteristics in early gadolinium shots (Figure 2, Panel G).
No signal enhancement in the 1st set of late acquisitions conforming its benign nature. Minimal enhancement at the very late set (>20 min) (Figure 2, Panels H-I).
The above CMR tissue characteristics are consisted with most likely a benign blood cyst arising from the endocardial layer of the mitral valve apparatus. Conservative management with routine serial imaging and no exercise restrictions were recommended. Our patient remained stable and active with no change in the size of lesion or the valvular function during echocardiographic surveillance.
Discussion
Primary cardiac tumors are rare and about 90% of them are benign [10]. Among benign cardiac masses, blood cysts seem to be even more uncommon and, as a matter of fact, they are rarely mentioned in literature reviews regarding cardiac tumors [10,11]. They are commonly found in autopsies of fetuses and infants below 2 months of age but, they constitute a scarce finding in older children [1], indeed, in a retrospective single-center review of patients < 21 years of age, diagnosed with a primary cardiac tumor between 1968 and 2010, only 2 in 178 patients were reported to have a blood cyst [12]. Patients are primarily asymptomatic since blood cysts are detected incidentally during routine echocardiographic assessment. Seldom, they can cause ventricular outflow obstruction or interfere with leaflet coaptation leading to valve regurgitation. Adult literature has associated blood cysts with embolic events, such as stroke or myocardial infraction, infective endocarditis, and rhythm disturbances [2]. Transthoracic echocardiography is the first line diagnostic approach, thanks to its low cost and its wide availability. It is usually adequate for the detection and localization of a cardiac mass, even of a small one, and can give useful information about function of the affected valve and possible obstructive phenomena. Transesophageal echocardiogram is an alternative option for detailed visualization of the valvular apparatus. Furthermore, with the use of latest enhancement agents, contrast echocardiogram can demonstrate attachment to the surrounding tissue and provide information regarding potential cardiac mass perfusion [10].
Yet, considering that other cardiac tumors may present with similar echocardiographic features with blood cysts, comprehensive multimodality imaging is often necessary to narrow down the differential diagnoses [2]. On Computed Tomography (CT) the cyst appears as a distinct non-enhancing hypodense lesion within the heart. Radiation exposure and lack of adequate tissue characterization limits the use of CT when infective endocarditis and extracardiac foci need to be excluded [13]. Cardiac Magnetic Resonance (CMR) offers precise information regarding the location of the lesion and its anatomic and functional relationship with the surrounding structures which is particularly valuable for pre-operative planning [12]. The diagnostic superiority of CMR refers to non-invasive tissue characterization of solid cardiac masses. Blood cysts appear hypo- or isointense on bSSFP and T1 weighted TSE with prolonged T1 relaxation time in inversion recovery sequences. Contrarily, they are significantly hyperintense in T2-weighted TSE sequences. The addition of a fat suppression pulse allows exclusion of fat containing tumors. Resting perfusion and early gadolinium enhancement are uncommon however, they are important in confirming absence of significant vascularity and differentiating from thrombi respectively. Occasionally, larger cysts with patent vascular channels may show late gadolinium enhancement due to rapid passage and sluggish removal of contrast; like our case that enhanced beyond 20 minutes post contrast administration. Undoubtedly, pathology remains the gold standard for accurately placing the diagnosis. Optimal management of asymptomatic patients with benign cardiac masses remains debatable. Literature is sparse regarding blood cyst risk stratification and planning. Surgical excision is recommended when valve dysfunction, obstructive or embolic phenomena occur, while conservative approach with echocardiographic surveillance is preferred for small asymptomatic cysts [14]. Few case reports on adult patients supported early surgical intervention to prevent potential complications [2-15]. However, this is a less preferrable strategy for young, small-sized patients with limited valve replacement options in case of procedural complications [8].
Conclusion
With our case presentation we opted to demonstrate the importance of multimodality imaging in the diagnosis of a solitary cardiac mass that is significantly rare among adolescents. A comprehensive CMR protocol is crucial to be able to differentiate with confidence between benign lesions and those that require immediate escalation of care. Interestingly, the mother of the patient had known history of excessive anterior mitral valve leaflet tissue that could suggest potential inheritability that has not been reported before. Considering the rarity of the diagnosis and lack of case series, management should be individualized according to age and clinical presentation.
References
- Zimmerman KG, Paplanus SH, Dong S, Nagle RB. Congenital blood cysts of the heart valves. Hum Pathol. 1983; 14(8): 699-703.
- Bortolotti U, Vendramin I, Lechiancole A, Sponga S, Pucci A, et al. Blood cysts of the cardiac valves in adults: Review and analysis of published cases. 2021; 36.
- Miles VN, Favara BE, Morriss JH, Prevedel AE, Hawes CR. Giant Blood Cyst and Congenital Pulmonic Stenosis: Report of a Case. American Journal of Diseases of Children. 1975; 129(9).
- Kuźma J, Rudziński A, Król W, Załuska-Pitak B, Oko-Łagan J, et al. Blood cyst attached to the anterior leaflet of the mitral valve. (RCD code: VI-1A.0). Journal of Rare Cardiovascular Diseases. 2016; 2(8).
- Ghawi H, Polimenakos AC, Gonzalez I, Abdulla R, Bokowski J. Giant pulmonary valve cyst in a 7-year-old child. Pediatr Cardiol. 2012; 33(4).
- Tan Recep BZ. A mitral blood cyst causing stenosis in the left ventricular outflow tract: A case report. Cardiovascular Surgery and Interventions. 2021; 8(2).
- Hsu JH, Wu JR, Chen HM, Huang WT. Stroke, infective endocarditis and a blood-filled cyst. Vol. 376, The Lancet. 2010.
- Karagözlü S, Ramoğlu MG, Dikmen Yaman N, Eyileten Z, Almus E. Giant intracardiac blood cyst of the mitral valve in a pediatric patient: A case report. Echocardiography. 2020; 37(6).
- Cianciulli TF, Ventrici JF, Marturano MP, Saccheri MC, Medus MJ, et al. Blood cyst of the mitral valve echocardiographic and magnetic resonance imaging diagnosis. Vol. 8, Circulation: Cardiovascular Imaging. 2015.
- Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, et al. Cardiac Tumors: JACC CardioOncology State-of-the-Art Review. 2020; 2.
- Bussani R, Castrichini M, Restivo L, Fabris E, Porcari A, et al. Cardiac Tumors: Diagnosis, Prognosis, and Treatment. 2020; 22.
- Miyake CY, Del Nido PJ, Alexander ME, Cecchin F, Berul CI, et al. Cardiac tumors and associated arrhythmias in pediatric patients, with observations on surgical therapy for ventricular tachycardia. J Am Coll Cardiol. 2011; 58(18).
- Beale RA, Russo R, Beale C, Levin W, Atalay MK, et al. Mitral Valve Blood Cyst Diagnosed with the Use of Multimodality Imaging. CASE. 2021; 5(3).
- Ludhwani D, Sheikh B, Sheikh Y. Evaluation of Mitral Apparatus Blood Cyst: A Case Report and Review of Literature. Cureus. 2019.
- Pasaoglu I, Dogan R, Nazli N, Gungen Y, Bozer AY. Blood cyst originating from tricuspid septal leaflet. Journal of Cardiovascular Surgery. 1991; 32(5).