
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Median rhomboid glossitis in an athlete: Report of a rare case
Matthieu Lefaux*; Grenie Yolène; Hirschauer François; Keletaona Youri; Vertu Nicolas
137th Medical Unit of Ventiseri Solenzara, 20240 Ventiseri, France.
*Corresponding Author : Matthieu Lefaux
137th Medical Unit of Ventiseri Solenzara, 20240 Ventiseri, France.
Email: matthieu.lefaux@def.gouv.fr
Received : Dec 16, 2024
Accepted : Jan 08, 2025
Published : Jan 15, 2025
Archived : www.jcimcr.org
Copyright : © Lefaux M (2025).
Abstract
We present a short report on the medical management of a young patient without any comorbidities coming with a typical median rhomboid glossitis. A detailed medical history revealed an unusual contributing factor, which appeared to lead to the development of this pathology.
Keywords: Median rhomboid glossitis; Good health patient; Dry mouth; Athlete.
Citation: Lefaux M, Grenie Y, Hirschauer F, Keletaona Y, Vertu N. Median rhomboid glossitis in an athlete: Report of a rare case. J Clin Images Med Case Rep. 2025; 6(1): 3425.
Introduction/background
Median rhomboid glossitis is a rare and still poorly understood disease, typically caused by an accumulation of Candida germs [1]. It accounts for 0.5% to 3% of all lingual lesions [2,3], and has a prevalence of approximately 0.01% to 0.1% in the general population. Males are more frequently affected than females [4]. The main recognized risk factors include immunosuppression [4,5], diabetes [5,6], and local conditions such as smoking or buccal microtrauma [2,5]. Due to its often-asymptomatic nature, median rhomboid glossitis is generally underdiagnosed. First medical management involves patient education focused on reducing or eliminating modifiable risk factors, along with the administration of topical antifungal medications [1,4].
Case presentation
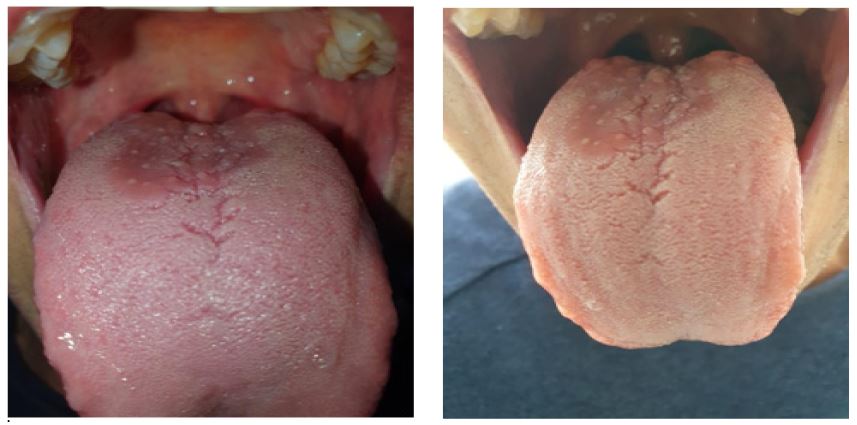
A 40-year-old patient is coming to our consultation with a centrally located depapillated lesion on the anterior part of the lingual V (Figure 1). It has been progressing over the past few weeks, along with a kissing lesion which is a corresponding lesion on the palatal vault (Figure 2). The patient is a non-smoker, has no significant medical history, and is not taking any medication. The lesion is asymptomatic. Clinically, no microtrauma that could increase the risk of pathological colonization by Candida has been identified.

Treatment and outcome
Given the typical clinical presentation, empirical treatment with nystatin oral suspension and baking soda mouth rinses was initiated. No laboratory tests or further exploration were done, following medical recommendations. Due to the persistence of symptoms after 10 days, biological tests were performed to investigate possible immunosuppression, and systemic antifungal therapy was introduced. The symptoms resolved completely after one month of treatment.
Discussion
In the absence of any previously identified risk factors in this young and athletic patient, and with laboratory results showing no signs of immunosuppression, a more specific medical interview was conducted. Among the many risk factors for Candida colonization, the only one identified for this patient was dry mouth. Indeed, we learned that the patient practiced snorkeling four times a week over the past several months. Snorkeling induces dry mouth due to prolonged mouth breathing which decreases salivary stimulation and limits hydration. All of this reduce saliva production and increase oral evaporation [7]. This persistent dry environment may have facilitated Candida colonization.
Conclusion
The most likely etiology of this median rhomboid glossitis contracted in a 40 years old patient with no comorbidity seems to be the repeated use of a snorkel, inducing dry mouth. The favorable response to systemic antifungal treatment and the cessation of symptoms following discontinuation of snorkeling leaded to a full recovery.
References
- Giovanna Pili FM, Erriu M, Piras A, Garau V. Application of the novel method in the diagnosis and treatment of median rhomboid glossitis Candida‑associated. European Journal of Dentistry. mars. 2014; 8: 129‑31.
- González-Álvarez L, García-Pola MJ. Risk factors associated with tongue lesions: a propensity score-matched case-control study. Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946. 2022; 1: 25-34.
- Goregena M, Miloglub O, Buyukkurtc MC, Caglayanb F, Aktasd AE. Median Rhomboid Glossitis: A Clinical and Microbiological Study. European Journal of Dentistry. 2011; 5: 367‑72.
- B Shinde, S Lohe, V Mohod, SV Dadgal, K Priya, et al. Median Rhomboid Glossitis of the Tongue-Associated Kissing Lesion: A Report of a Rare CaseShinde. Cureus. 2024.
- amaranayake L, Keung Leung W, Jin L. Oral mucosal fungal infections. Periodontology 2000. 2009; 39‑59.
- Ghabanchi J, Andisheh Tadbir A, Darafshi R, Sadegholvad M. The Prevalence of Median Rhomboid Glossitis in Diabetic Patients: A Case-Control Study. Iranian Red Crescent Medical Journal. 2011; 13.
- Ramirez-Yanez German O. Mouth Breathing: Understanding the Pathophysiology of an oral habit and its consequences. Medical Research Archives, European society of medicine. [Online] 2022; 11(1).