
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Foveolar-sparing arterial branch occlusion in a young woman with mitral valve disease
AW Aïssatou*; SY El Hadji Malick; Mbaye Soda; KA Aly Mbara; Diagne JP; Diallo Hawo Madina; Samra Audrey; Ndiaye Papa Amadou4
Ophthalmology Center of Abass Ndao Hospital, Dakar, Senegal.
*Corresponding Author : Aïssatou AW
Ophthalmology Center of Abass Ndao Hospital, Dakar, Senegal.
Email: aichatou18@gmail.com
Received : Dec 16, 2024
Accepted : Jan 09, 2025
Published : Jan 16, 2025
Archived : www.jcimcr.org
Copyright : © Aïssatou AW (2025).
Abstract
Purpose: To report the case of a unilateral retinal arterial branch occlusion (OBAR) in a young woman with a history of surgically treated miltral valve pathology.
Observation: This was a 39-year-old patient with a history of mitral stenosis treated by commissurotomy. She presented with a 2-day history of upper visual field amputation. Examination showed corrected visual acuity of 10/10e P2 in both eyes, with normal anterior segment and ocular tone. The fundus on the left showed inferior retinal ischemic edema sparing the foveolar region, with an embolus at the emergence of the inferior temporal branch also visible on fluorescence angiography. Optical coherence tomography showed sectorial thickening of the inner layers. Doppler ultrasound of the supra-aortic trunks was normal. Echocardiography showed moderate dilatation of the thrombus-free left atrium, with thickened, remodelled mitral valves. After 8 months’ follow-up, his visual acuity remained unchanged, with a superior scotoma at visual field.
Discussion: Retinal artery occlusions in young adults is rare, few cases are reported in the literature. Unlike adults where atheromatous pathology is the most incriminated, in young people cardiac causes are the most frequent.
Conclusion: Retinal arterial branch occlusion is an ophthalmological emergency whose prognosis depends on the condition of the macula. Its occurrence in young patients calls for a rigorous etiological approach.
Keywords: Retinal artery occlusion; Embolus; Mitral valve.
Citation: Aïssatou AW, Malick SYEH, Soda M, Mbara KAA, Diagne JP, et al. Foveolar-sparing arterial branch occlusion in a young woman with mitral valve disease. J Clin Images Med Case Rep. 2025; 6(1): 3426.
Introduction
Branch Retinal Artery Occlusions (BRAOs) account for an estimated 38% of all retinal artery occlusions [1]. In the literature, all retinal artery occlusions are often grouped together, which explains the scarcity of data specific to branch artery occlusion [2]. They may be secondary to mechanical or inflammatory obstruction of a branch of the central retinal artery. Visual field deficit depends on the area of non-perfusion, which may or may not include the macula [1]. 60-70% of cases, an embolus is detected, and 90% of cases, it is located at a bifurcation of the temporal branches [3]. BRAO remains a rare condition in young, and the prognosis depends on the degree of arterial repermeabilization and the causative pathology. We report an branch retinal artery occlusion with foveolar sparing in a young woman with mitral valve disease.
Observation
This was a 39-year-old melanoderma patient with a history of mitral stenosis diagnosed in 2003 and treated by commissurotomy without anticoagulant therapy.
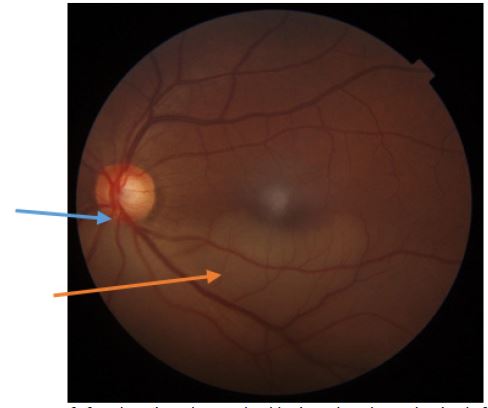
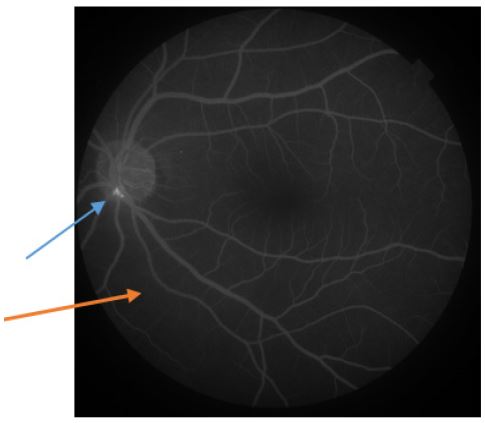
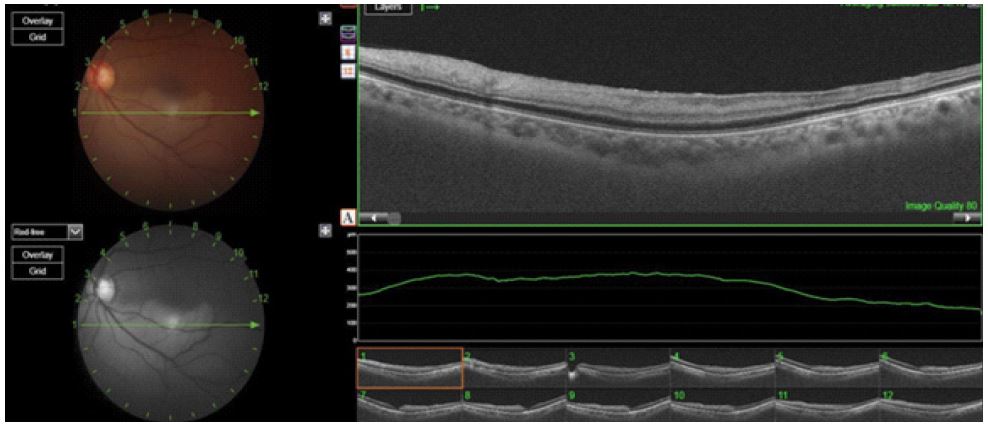
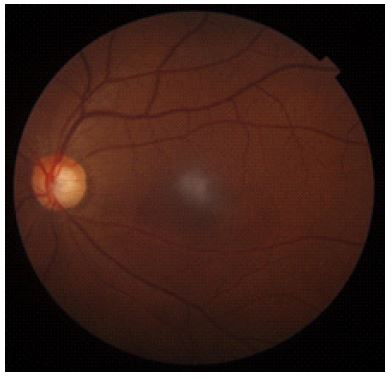
She had undergone an emergency consultation for an upper visual field amputation that had appeared 2 days previously. Examination showed corrected visual acuity of 20/20 Parinaud 2 in both eyes, with normal anterior segment and intra ocular pressure. Fundus examination was normal on the right, and showed inferior ischemic edema on the left, sparing the foveolar region, with an embolus at the emergence of the inferior temporal branch. Fluorescein angiography showed the presence of a hyperfluorescent embolus at the emergence of the inferior temporal branch, with repermeabilization and capillary hypo-perfusion inferiorly. Optical Coherence Tomography (OCT) showed a sectorial thickening of the inner retinal layers without any change in macular thickness, with integrity of the outer retinal layers. She was referred to her attending cardiologist for an assessment of her pathology. Doppler ultrasound of the supra-aortic trunks was normal.
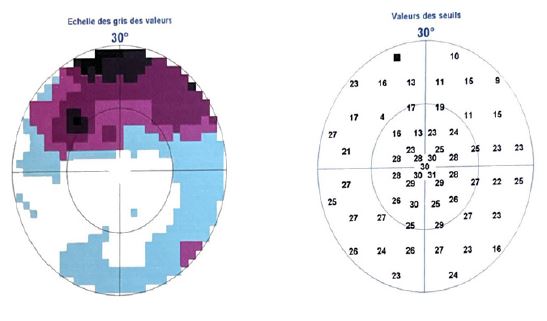
Echocardiography showed moderate dilatation of the thrombus-free left atrium, with thickened, remodelled mitral valves of limited aperture and moderate involvement of the subvalvular apparatus. Lipid profile was normal. After 8 months’ follow-up, his visual acuity remained preserved, with a superior scotoma visible in visual field test.
Discussion
BRAO predominates in men, with a higher frequency in people over 60 years [4]. In the series of 52 patients by Mason et al. [5], the mean age was 65, with no gender predilection. Hayreh et al. [6] reported a male predominance (65%) with an average age of 59. This is a rare pathology in young subjects. In our case, the patient was 39 years old.
Symptoms are sudden and painless decreased visual acuity. BRAO generally manifests itself as an amputation of the horizontal visual field, although central vision may be preserved [4], as in our patient’s case. Ischemic edema may involve the macula, leading to a reduction in visual acuity, but less severe than in occlusion of the central retinal artery, and an absence of macular involvement is a form of better prognosis, with preserved visual acuity. Ischemic edema may resolve during the course of the disease. In the series by Hayreh et al. [7], 34% of cases, the edema persisted after 1 month, and en 13% after 3 months. In our case, retinal ischemic edema had disappeared after 8 months. The temporal location of the occlusion in our observation appears to be the most frequent location of BRAO, however, it has not been demonstrated that this very high frequency corresponds to hemodynamic phenomena specific to this vascular network [4]. In a series of 136 eyes with BRAO, the location was superior temporal in 29% of cases and inferior temporal in 26% [7]. It has been reported that occlusion of nasally distributed branches has no significant functional consequences and remains only mildly symptomatic for patients, who do not necessarily consult and are therefore largely underestimated [1,4]. En 60-70% of cases, an embolus is detected and, 90% of cases, localized at a bifurcation of the temporal branches, without any hemodynamic phenomena specific to this network having been demonstrated. Hayreh et al. found this to be the case en 65% of their patients [7]. In our patient, the embolus, visible on fundus and fluorescein angiography, was located at the emergence of the inferior temporal branch. In addition, the migration and fragmentation of these emboli by activation of endogenous fibrinolysis often make them difficult to detect. Direct examination during the chronic phase of repermeabilization reveals the affected territory with great difficulty and resolution of the edema, so that the real incidence of BRAO linked to emboli appears to be underestimated, with normal retinal perfusion on angiography. Eyes with BRAO show different degrees of retinal ischemic damage, depending on the duration of vascular obstruction and the degree of impaired blood flow. It has been reported that the degree of capillary non-perfusion detected by OCT-A correlates with the degree of retinal ischemic damage to the microvascular structure in OCT images [8]. Unlike subjects over 50, where atheromatous pathology is the main cause of retinal artery occlusion, in subjects under 45, cardiac pathologies predominate [1]. Greven et al. [9] reported 21 cases of patients under 40 with retinal artery occlusion. They found that cardiac valvular disease was present in 19% of cases, and that in 91% of cases, various associated factors led to a hypercoagulable or embolic state. They concluded that retinal artery occlusions in young adults occur via multiple mechanisms. In the series by Hayreh et al. [6], of 42% artery occlusions with embolic origin, 31% originated from the mitral valve, 28% from the aortic valve and 41% from both valves. Mitral valve lesions included 70% calcified valves, 4% valve prolapse and 26% with other types of lesion. In our case, the echocardiogram showed moderate dilatation of the thrombus-free left atrium, with thickened, remodelled mitral valves of limited aperture and moderate damage to the subvalvular apparatus. The condition of the mitral valves could be implicated in the formation of the embolus responsible for the BRAO in the left eye. Mason et al. [5] had assessed the visual prognosis of patients with BRAO, eyes with a VA of 20/40 or better generally remained at 20/40 or better, and those with a poor VA of 20/100 or less generally showed no significant improvement. They then concluded that visual prognosis after BRAO appeared to be correlated with initial VA. In BRAO, even in the case of foveolar sparing, visual field damage generally persists [4], as in the case of our patient, who had a superior scotoma. However Ros et al. [10] report that among 123 eyes with BRAO, 33% had almost complete resolution of their scotomas, and 66% of eyes had persistent deficits.
Conclusion
repermeabilization reveals the affected territory with great difficulty and resolution of the edema, so that the real incidence of BRAO linked to emboli appears to be underestimated, with normal retinal perfusion on angiography. Eyes with BRAO show different degrees of retinal ischemic damage, depending on the duration of vascular obstruction and the degree of impaired blood flow. It has been reported that the degree of capillary non-perfusion detected by OCT-A correlates with the degree of retinal ischemic damage to the microvascular structure in OCT images [8]. Unlike subjects over 50, where atheromatous pathology is the main cause of retinal artery occlusion, in subjects under 45, cardiac pathologies predominate [1]. Greven et al. [9] reported 21 cases of patients under 40 with retinal artery occlusion. They found that cardiac valvular disease was present in 19% of cases, and that in 91% of cases, various associated factors led to a hypercoagulable or embolic state. They concluded that retinal artery occlusions in young adults occur via multiple mechanisms. In the series by Hayreh et al. [6], of 42% artery occlusions with embolic origin, 31% originated from the mitral valve, 28% from the aortic valve and 41% from both valves. Mitral valve lesions included 70% calcified valves, 4% valve prolapse and 26% with other types of lesion. In our case, the echocardiogram showed moderate dilatation of the thrombus-free left atrium, with thickened, remodelled mitral valves of limited aperture and moderate damage to the subvalvular apparatus. The condition of the mitral valves could be implicated in the formation of the embolus responsible for the BRAO in the left eye. Mason et al. [5] had assessed the visual prognosis of patients with BRAO, eyes with a VA of 20/40 or better generally remained at 20/40 or better, and those with a poor VA of 20/100 or less generally showed no significant improvement. They then concluded that visual prognosis after BRAO appeared to be correlated with initial VA. In BRAO, even in the case of foveolar sparing, visual field damage generally persists [4], as in the case of our patient, who had a superior scotoma. However Ros et al. [10] report that among 123 eyes with BRAO, 33% had almost complete resolution of their scotomas, and 66% of eyes had persistent deficits.
References
- Pierru A, Roemer S, Paques M. Occlusions artérielles rétiniennes. EMC - Ophtalmologie. 2021; 38(4): 1-10.
- Hayreh SS, Podhajsky PA, Zimmerman MB. Branch Retinal Artery Occlusion. Ophthalmology. 2009; 116: 1188-1194.4.
- Shah GK, Sharma S, Brown GC. Iris neovascularization following branch retinal artery occlusion. Can J Ophthalmol. 1998; 33: 389‑90.
- Pournaras CJ. Ocular vascular disease. Elsevier Masson. 2008; 22: 537-39.
- Mason JO, Shah AA, Vail RS, Nixon PA, Ready EL, et al. Branch Retinal Artery Occlusion: Visual Prognosis. Am J Ophthalmol. 2008; 146: 455‑7.
- Hayreh SS, Podhajsky PA, Zimmerman MB. Retinal artery occlusion: Associated systemic and ophthalmic abnormalities. Ophthalmology. 2009; 116: 1928‑36.
- Hayreh SS, Zimmerman MB. Fundus changes in branch retinal arteriolar occlusion. Retina. 2015; 35: 2060‑6.
- Igawa Y, Amaki H, Kanno J, Tachibana M, Konno S, et al. Evaluations of microvascular density by optical coherence tomography, angiography, and function by multifocal electroretinography of the macular area in eyes with branch retinal artery occlusion. Front Ophthalmol. 2023; 3: 1255098.
- Greven CM, Slusher MM, Weaver RG. Retinal arterial occlusions in young adults. Am J Ophthalmol. 1995; 120: 776‑83.
- Ros MA, Magargal LE, Uram M. Branch retinal-artery obstruction: A review of 201 eyes. Ann Ophthalmol. 1989; 21: 103‑7.