
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Cerebellopontine angle schwannoma with obstructive hydrocephalus causing posterior disc bulge of spinal cord: A rare clinical image
Vishal Telrandhe1; Ruchika Zade2; Sharath Hullumani V3*
1UG Scholar, Department of Paediatric Physiotherapy, Ravi Nair Physiotherapy college, Datta Meghe Institute of Higher Education and Research (DU), Sawangi (Meghe), Wardha, Maharashtra, India.
2Resident, Department of Neurophysiotherapy, Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research (DU), Sawangi (Meghe), Wardha, India.
3Assistant Professor, Department of Paediatric Physiotherapy, Ravi Nair Physiotherapy College, Datta Meghe Institute Higher Education and Research (DU), Sawangi (Meghe), Wardha, India.
*Corresponding Author : Sharath Hullumani V
Assistant Professor, Department of Paediatric Physiotherapy, Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research (DU), Sawangi (Meghe), Wardha, India.
Tel: +91 9964066927;
Email: sharathhullumani@gmail.com
Received : Dec 16, 2024
Accepted : Jan 10, 2025
Published : Jan 17, 2025
Archived : www.jcimcr.org
Copyright : © Hullumani VS (2025).
Abstract
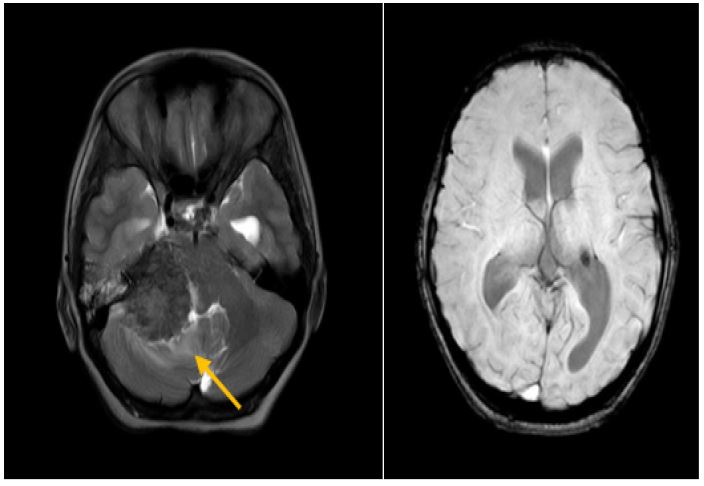
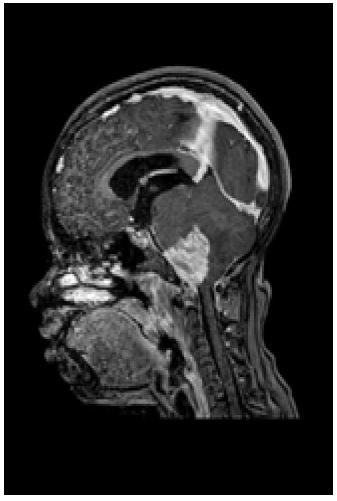
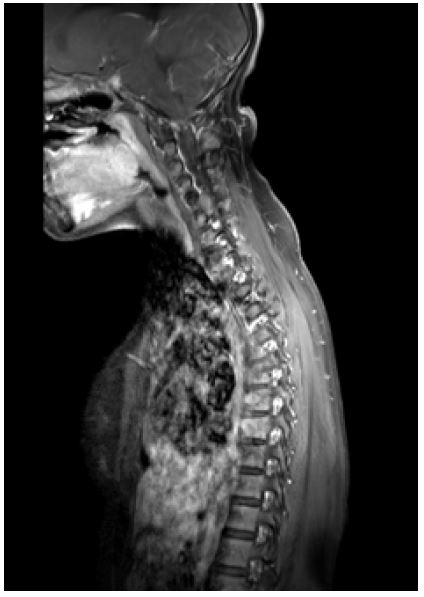
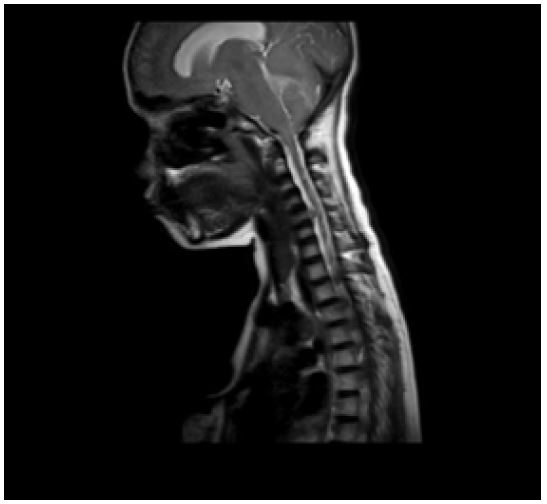
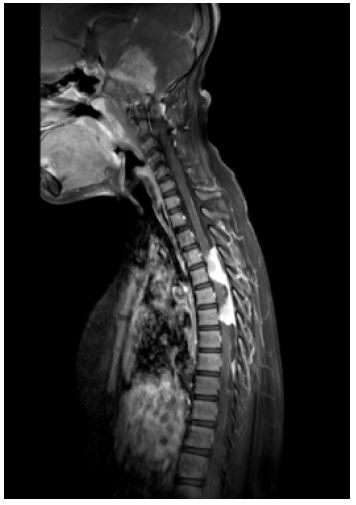
A 14-year-old girl complained of weakness in both lower limbs and balance issues with hypotonic tone in both lower limbs. Knee and ankle jerk reflexes were absent in both lower limbs, although plantar response extensor bilaterally grade 1 clonus was present in the right lower limb. Investigation were done like Magnetic Resonance Imaging (MRI) of brain which reveled that right CP angle schwannoma size 4.5 x 4 x 3.5 cm causing obstructive hydrocephalus brainstem rotated, fourth ventricle is effaced and the lesion shows perilesional edema with neurofibroma 6 x 5 x 4 cm medial to right parotid, multiple plaque like nodular intraspinal meningiomas seen at anterior epidural space at C5 level. Nodular pachymeningeal enhancement is seen in the cervical level. Nodular enhancement is seen in the right parasellar and suprasellar region. Magnetic Resonance Imaging (MRI) whole spine revealed that posterior disc bulge causing thecal sac indentation in seen involving C3-C4, C4-C5, and C5-C6 levels. Lobulated intensely enhancing Dural based masses are seen in the spinal canal at D3-D4 (32 x 15 mm), D5-D6 (24 x 16 mm), and at the D8-D9 (23 x 6 mm) level.
Citation: Telrandhe V, Zade R, Hullumani VS. Cerebellopontine angle schwannoma with obstructive hydrocephalus causing posterior disc bulge of spinal cord: A rare clinical image. J Clin Images Med Case Rep. 2025; 6(1): 3428.
Introduction
A 14-year-old girl complained of weakness in both lower limbs and balance issues with hypotonic tone in both lower limbs. Knee and ankle jerk reflexes were absent in both lower limbs, although plantar response extensor bilaterally grade 1 clonus was present in the right lower limb. Investigation was done like Magnetic Resonance Imaging (MRI) of brain which revealed that right CP angle schwannoma size 4.5 x 4 x 3.5cm causing obstructive hydrocephalus brainstem rotated, fourth ventricle is effaced and the lesion shows perilesional edema with neurofibroma 6 x 5 x 4 cm medial to right parotid, multiple plaque like nodular intraspinal meningiomas seen at anterior epidural space at C5 level. Nodular pachymeningeal enhancement is seen in the cervical level. Nodular enhancement is seen in the right parasellar and suprasellar region. Magnetic Resonance Imaging (MRI) whole spine revealed that posterior disc bulge causing thecal sac indentation in seen involving C3-C4, C4-C5, and C5-C6 levels. Lobulated intensely enhancing Dural based masses are seen in the spinal canal at D3-D4 (32 x 15 mm), D5-D6 (24 x 16 mm), and at the D8-D9 (23 x 6 mm) level. The symptomatic accumulation of Cerebrospinal Fluid (CSF) in side the brain ventriclees is known as hydrocephalus [1]. This buildup could be caused by a blockage in the CSF’s normal flow, a difficulty with the Pacchionian arachnoid granulations’ ability to absorb CSF into the venous system, or an excessive amount of CSF being produced. Early in 1913, Dandy offered the first classifications for hydrocephalus: communicative and non-communicating (obstructive) [2,3]. Since then, numerous additional categories have been presented. Obstructive, communicative, hypersecretory, and Normal Pressure Hydrocephalus (NPH) are the four forms that affect adults. A genetic condition or spinal dysraphism is frequently associated with congenital or developmental hydrocephalus, which is frequently evident at birth [4]. An obstruction in the CSF channels leads to obstructive hydrocephalus [5]. The foramina Monro, the aqueduct of Sylvius, the fourth ventricle, and the foramen magnum are the locations where the obstruction occurs most frequently, however most tumors of a size that is significant can obstruct at any point of the CSF pathways. Ependymoma, subependymal giant cell astrocytoma, choroid plexus papilloma, craniopharyngioma, pituitary adenoma, hypothalamic or optic nerve glioma, hamartoma, and metastatic cancers are a few of the most common malignancies linked to hydrocephalus. Hydrocephalus development is frequently linked to posterior fossa tumors [6]. Impaired CSF absorption leads to communicating hydrocephalus. Post-hemorrhagic or post-inflammatory alterations are the most frequent causes. One-third of these instances are attributable to subarachnoid bleeding, which prevents CSF absorption at the arachnoid granulations [7].
References
- Rojas R, Riascos R, Vargas D, Cuellar H, Borne J. Neuroimaging in drug and substance abuse part I: Cocaine, cannabis, and ecstasy. Top Magn Reson Imaging. 2005; 16(3): 231-8.
- Holt JL, Kraft-Terry SD, Chang L. Neuroimaging studies of the aging HIV-1-infected brain. J Neurovirol. 2012; 18(4): 291-302.
- Pini L, Pievani M, Bocchetta M, Altomare D, Bosco P, et al. Brain atrophy in Alzheimer’s Disease and aging. Ageing Res Rev. 2016; 30: 25-48.
- Kim H, Jeong EJ, Park DH, Czosnyka Z, Yoon BC, et al. Finite element analysis of periventricular lucency in hydrocephalus: extravasation or transependymal CSF absorption? J Neurosurg. 2016; 124(2): 334-41.
- LeMay M, Hochberg FH. Ventricular differences between hydrostatic hydrocephalus and hydrocephalus ex vacuo by computed tomography. Neuroradiology. 1979; 17(4): 191-5.
- Kahlon B, Annertz M, Ståhlberg F, Rehncrona S. Is aqueductal stroke volume, measured with cine phase-contrast magnetic resonance imaging scans useful in predicting outcome of shunt surgery in suspected normal pressure hydrocephalus? Neurosurgery. 2007; 60(1): 124-9; 129-30.
- Larsson A, Moonen M, Bergh AC, Lindberg S, Wikkelsö C. Predictive value of quantitative cisternography in normal pressure hydrocephalus. Acta Neurol Scand. 1990; 81(4): 327-32.