
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
A case of cerebral edema following hypernatremia correction
Jumpei Otsuka1 ; Yoshinao Ono2 *; Katsuya Takita2 ; Ryutaro Suzuki3
1Department of Respiratory Medicine, Kesennuma City Hospital, 8-2, Akaiwasuginosawa, Kesennuma, Miyagi 988-0181, Japan.
2Department of Respiratory Medicine, Tohoku University Graduate School of Medicine, 1-1, Seiryomachi, Aobaku, Sendai, Miyagi 980-8574, Japan.
3Department of Neurosurgery, Tohoku University Graduate School of Medicine, 1-1, Seiryomachi, Aobaku, Sendai, Miyagi 980- 8574, Japan.
*Corresponding Author : Yoshinao Ono
Department of Respiratory Medicine, Tohoku
University Graduate School of Medicine, 1-1,
Seiryomachi, Aobaku, Sendai, Miyagi 980-8574,
Japan.
Tel: +81- 22-717-8539;
Email: yoshinao.ono.a8@tohoku.ac.jp
Received : Dec 29, 2024
Accepted : Jan 14, 2025
Published : Jan 21, 2025
Archived : www.jcimcr.org
Copyright : © Ono Y (2025).
Keywords: Empagliflozin; Cerebral edema; Hypernatremia.
Citation: Otsuka J, Ono Y, Takita K, Suzuki R. A case of cerebral edema following hypernatremia correction. J Clin Images Med Case Rep. 2025; 6(1): 3433.
Description
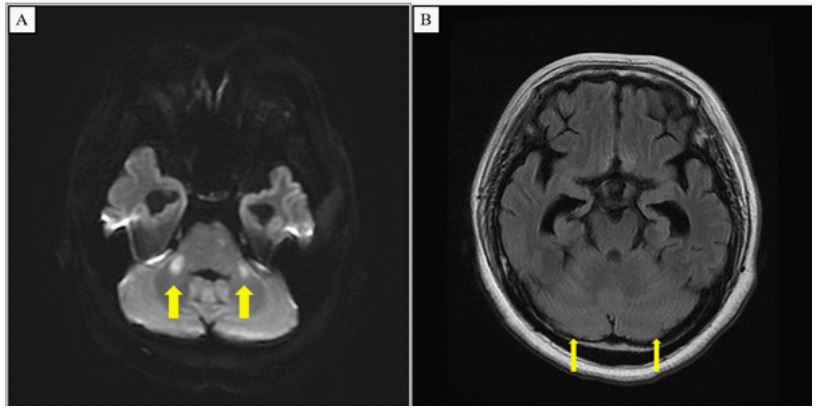
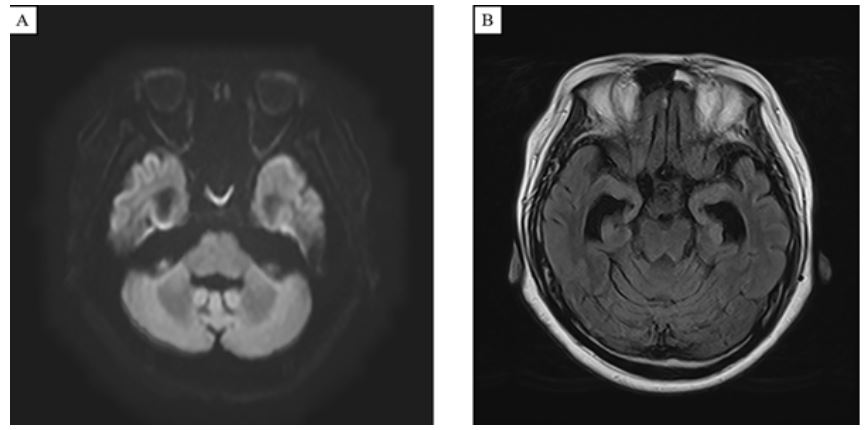
A 52-year-old woman with mental retardation and diabetes mellitus was hospitalized for a bronchial asthma attack. As the wheezing subsided with dexamethasone, empagliflozin was restarted on the second day, leading to polyuria and an increase in serum sodium to 191 mEq/L by the fourth day. Following discontinuation of empagliflozin, her Na level dropped to 145 mEq/L by the 11th day, but she remained unsteady. On the 13th day, a head Magnetic Resonance Imaging (MRI) showed high-signal areas in the middle cerebellar peduncles on diffusion-weighted images and disappearance of cerebral sulci on fluid-attenuated inversion recovery, suggesting cerebral edema due to hypernatremia correction (Figure 1). Her symptoms improved with rehabilitation, and a repeat MRI on the 30th day showed resolution (Figure 2). In adults, it is generally recommended that hypernatremia correction should not exceed 12 mEq/L per day [1]. However, this guideline is derived from observational studies in infants and children, with limited direct evidence in adults. Reports suggest that even when sodium levels are corrected faster than 12 mEq/L per day in adults, no consistent associations with mortality, seizures, altered consciousness, or cerebral edema have been observed [2]. Nevertheless, slow correction of hypernatremia in adults may be prudent to minimize potential risks.
References
- Kim SW. Hypernatemia: Successful treatment. Electrolyte Blood Press. 2006; 4: 66-71.
- Chauhan K, Pattharanitima P, Patel N, et al. Rate of Correction of Hypernatremia and Health Outcomes in Critically Ill Patients. Clin J Am Soc Nephrol 2019; 14: 656-63.