Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Splenic lymphangioma: Clinical image
*Corresponding Author : Beatriz Porteiro
Department of Internal Medicine, Professor Doutor Fernando Fonseca Hospital, Amadora, Portugal.
Email: beatriz.porteiro@ulsasi.min-saude.pt
Received : Dec 27, 2024
Accepted : Jan 16, 2025
Published : Jan 23, 2025
Archived : www.jcimcr.org
Copyright : © Porteiro B (2025).
Citation: Porteiro B. Splenic lymphangioma: Clinical image. J Clin Images Med Case Rep. 2025; 6(1): 3436.
Description
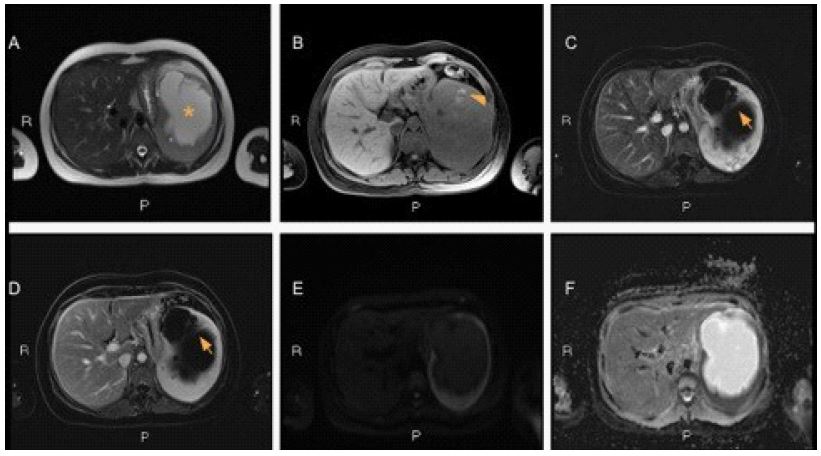
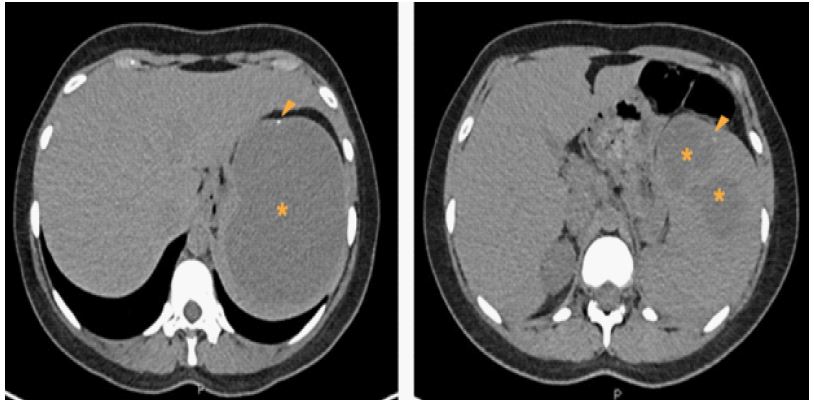
A 25 years-old woman presented to the emergency department with persistent left flank abdominal pain with dorsal irradiation after a 7 days cefuroxime course prescribed for acute pyelonephritis. She had no prior history of abdominal trauma. On abdominal examination she had left quadrant tenderness and pain elicited by percussion in the kidney area. An abdominal US complemented by a CT-scan (Figure 1) found a well-circumscribed multiloculated splenic cystic measuring 11,1 x 10 x 8,5 cm with homogeneous hypodense fluid content (*) and small peripheral calcifications (arrow heads). Serological examinations rule out parasitic etiology and CA19-9 level was normal. A MRI (Figure 2) showed a multiloculated cyst (A,*) with small proteinaceous/hematic component within it (B, arrow head), and slight enhancement of the lesion’s septations at fat suppressed T1IW, with no solid component seen (C, arrows). The lesion has low signal intensity in DWI b900 (E) and high values on ADC map (F). A splenic lymphagioma, a rare congenital splenic tumor, was suspected and therefore splenectomy was proposed.