
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Acral lentiginous melanoma and renal cell carcinoma: A rare association
Ghita Basri1*; I Chikhaoui1; S Nejjari1; M El Omari2; M Kharbouch2; M Mahi3; A Al Bouzidi4; F Agharbi1; S Chiheb1-5
1Department of Dermatology, International University Hospital Cheikh Khalifa, Faculty of Medicine, Mohammed VI University of Health Sciences, Morocco.
2Department of Plastic, Reconstructive, and Aesthetic Surgery, International University Hospital Cheikh Khalifa, Faculty of Medicine, Mohammed VI University of Health Sciences, Morocco.
3Department of Radiology, International University Hospital Cheikh Khalifa, Faculty of Medicine, Mohammed VI University of Health Sciences, Morocco.
4Department of Pathology, International University Hospital Cheikh Khalifa, Faculty of Medicine, Mohammed VI University of Health Sciences, Morocco.
5Department of Dermatology, Ibn Rochd University Hospital, Faculty of Medicine, Hassan II University, Morocco.
*Corresponding Author : Ghita Basri
Department of Dermatology, International University Hospital Cheikh Khalifa, Faculty of Medicine, Mohammed VI University of Health Sciences, Morocco.
Email: ghitabas@outlook.fr
Received : Nov 15, 2024
Accepted : Jan 20, 2025
Published : Jan 27, 2025
Archived : www.jcimcr.org
Copyright : © Basri G (2025).
Citation: Basri G, Chikhaoui I, Nejjari S, Omari MEI, Kharbouch M, et al. Acral lentiginous melanoma and renal cell carcinoma: A rare association. J Clin Images Med Case Rep. 2025; 6(1): 3441.
Introduction
Melanoma is a malignant skin tumor that originates from melanocytic cells. The coexistence of melanoma and clear cell renal carcinoma is a rare occurrence. We present a new case.
Case report
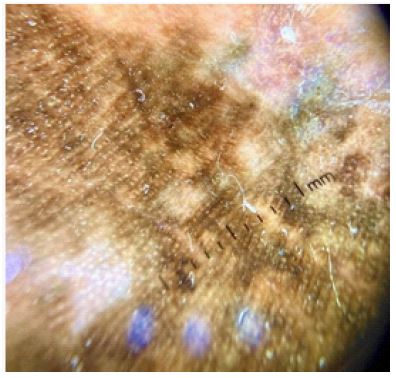
A 75-year-old patient, with no medical history, presented with a heterogeneous pigmented plaque featuring a central ulceration that bled on touch. The lesion measured 6 x 6 cm, was irregularly shaped, asymmetrical, with poorly defined and uneven borders (Figure 1). The dermoscopic examination of the plantar skin lesion revealed the following morphological features: Asymmetric pigmentation, irregular vascular structures, and features such as rhomboid blotches, a negative pigment network, blue-gray veils, and atypical globules. Excisional biopsy with immediate histopathological examination revealed an acral lentiginous melanoma. The patient underwent reconstructive surgery with a flap. During staging investigations, a renal mass was discovered, which appeared malignant on CT and showed increased uptake on PET-CT (Figure 3). A CT-guided biopsy confirmed the diagnosis of clear cell renal carcinoma.


Discussion
Melanoma is known to be a highly metastatic cutaneous tumor. However, the association between melanoma and another malignancy, particularly renal carcinoma, is extremely uncommon [1]. The genetic anomaly responsible for this association is a missense germline mutation in the MITF gene (microphthalmia-associated transcription factor). MITF plays a crucial role in melanocyte homeostasis and has recently been linked to melanoma pathogenesis, as well as to the regulation of certain target factors implicated in the predisposition to kidney cancer [2,3]. This case is notable not only for its rarity but also for the importance of raising awareness among dermatologists and other clinicians about the need for early detection. Thus, the diagnosis of melanoma should prompt consideration of potential renal involvement, in addition to the standard staging procedures. This highlights the importance of radiological assessments to detect secondary sites and the role of CT- guided biopsy to confirm the tumor’s histological type. Similarly, the presence of a renal tumor should alert the clinician to the possibility of suspicious pigmented skin lesions, which can improve the chances of successful treatment. Unfortunately, genetic testing for this mutation was not performed in our case due to resource limitations. The patient has since been referred to the urology department for management of the renal tumor and is scheduled for curative surgery.
Conclusion
Managing patients with both melanoma and renal cancer remains challenging, given the high mortality rates associated with each cancer individually, as well as the often complex multi-pathological nature of such cases.
References
- Kim K, Chung TH, Etzel CJ, Kim J, Ryu H, et al. Association between melanoma and renal- cell carcinoma for sequential diagnoses: A single-center retrospective study. Cancer Epidemiol. 2018; 57: 80‑ 4.
- Maubec E, Chaudru V, Mohamdi H, Grange F, Patard JJ, et al. Characteristics of the coexistence of melanoma and renal cell carcinoma. Cancer. 2010; 116(24): 5716‑ 24.
- Abern MR, Tsivian M, Coogan CL, Kaufman HL, Polascik TJ. Characteristics of patients diagnosed with both melanoma and renal cell cancer. Cancer Causes Control CCC. 2013; 24(11): 1925‑ 33.