
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Accelerated rheumatoid nodulosis effectively treated with JAK-inhibitors: A description of 2 cases and review of literature
Calvisi SL1*†; Farina N1†; Baldissera E1; Boffini N1; Cariddi A1; Tomelleri A1,2; Cinalli S3; Matucci-Cerinic M1; Dagna L1,2
1Unit of Immunology, Rheumatology, Allergy and Rare Diseases, IRCCS San Raffaele Hospital, Milan, Italy.
2School of Medicine, Vita-Salute San Raffaele University, Milan, Italy.
3Department of Pathology, ASST Valtellina and Alto Lario, Sondrio, Italy.
#Equal Contribution.
*Corresponding Author : Calvisi SL
Unit of Immunology, Rheumatology, Allergy and Rare Diseases, IRCCS San Raffaele Hospital, Milan, Italy.
Email: calvisi.stefania@hsr.it
Received : Dec 09, 2024
Accepted : Jan 21, 2025
Published : Jan 28, 2025
Archived : www.jcimcr.org
Copyright : © Calvisi SL (2025).
Abstract
Rheumatoid Nodules (RN) are the most common extra-articular manifestation of rheumatoid arthritis (RA), while Accelerated Rheumatoid Nodulosis (ARN) is a rare event potentially triggered by immunosuppressive therapies. ARN management is not standardized: removing the causative drug towards an alternative treatment is the most common implemented strategy. Recently, Janus Kinase inhibitors (JAKi) have attained a crucial role for disease control in multidrug-resistant RA patients. Herein, we describe two cases of extensive subcutaneous and pulmonary ARN associated with tocilizumab and etanercept therapies, both resolved after a swap to filgotinib monotherapy. We also provide a narrative literature review, supporting the usefulness of JAKi in controlling this difficult-to- treat complication.
Keywords: Rheumatoid arthritis; Rheumatoid nodules; JAK inhibitors.
Citation: Calvisi SL, Farina N, Baldissera E, Boffini N, Cariddi A, et al. Accelerated rheumatoid nodulosis effectively treated with JAK-inhibitors: A description of 2 cases and review of literature. J Clin Images Med Case Rep. 2025; 6(1): 3443
Introduction
Rheumatoid Nodules (RN) are detected in 20-30% of Rheumatoid Arthritis (RA) patients [1] and may present as Classic Rheumatoid Nodules (CRN), rheumatoid nodulosis, or Accelerated Rheumatoid Nodulosis (ARN) [2,3]. ARN has been reported in patients treated with conventional synthetic or biologic disease- modifying antirheumatic drugs (cs/bDMARDs) such as Methotrexate (MTX) [3-5], Leflunomide (LFN) [6], azathioprine [7], anti-TNFα agents [8-14], and anti-interleukin-6 therapies [15,16]. The term “accelerated” refers to the rapid onset and progression or to the extension of pre-existing nodules. The interval between the starting of the culprit drug and the development of nodules ranges from weeks to years and is unrelated to cumulative drug dosage. ARN often occurs in patients whose arthritis is in remission, unlike CRN.
CRN are usually located subcutaneously in areas of external pressure (e.g., elbows) but may also form in internal organs under mechanical stress (e.g., lungs, heart, larynx, liver, eyes, meninges, bladder), causing local damage. In ARN, the nodules are smaller but clinically similar to those seen in CRN, and they tend to develop on extremities (e.g., hands, feet) [2]. Pathologically, RN in ARN and CRN share similar granulomatous features [17,18] and risk factors [5,19-21]. Regional inflammation due to local trauma contributes to CRN pathogenesis [1], whereas ARN is primarily related to ongoing medications [4-16,19,20]. RN are associated with more severe systemic disease, particularly in ARN, a condition often symptomatic and occasionally life-threatening [21].
While CRN treatment is typically unnecessary, surgical removal may be required in cases of infection or local mass effects. ARN generally resolved by discontinuing the precipitating drug, sometimes with additional therapies [5,15,16,22-25]. This report describes two cases of subcutaneous and pulmonary ARN efficaciously treated with Janus Kinase inhibitors (JAKi) and reviews seven other cases in which JAKi were successfully employed [26-32].
Case series
Case 1
In February 2024, a 62-year-old woman with a 16-year history of seropositive erosive RA, and a carrier of the HLA-DRB1*0401 allele, presented with the rapid onset of multiple subcutaneous nodules on her feet, with no prior history of RN. Physical examination revealed indurated, tender, erythematous subcutaneous nodules on the lateral margins of both feet, ranging from one to several centimeters in size. Ultrasound (US) imaging showed mixed, lobulated, inhomogeneous, hypoechoic, and non-compressible masses near the bone surfaces, with a central anechoic area and diffuse peripheral Doppler signals (Figure 1a). MRI confirmed typical RN features: low signal on T1-weighted and high signal on T2- weighted images, hyperintense STIR sequences, and reactive edema in surrounding adipose tissue (Figure 1b). The patient had previously been treated with LFN, sulfasalazine, MTX, certolizumab pegol, upadacitinib, and baricitinib, all discontinued due to inefficacy or toxicity. Tocilizumab was initiated two months before the ARN developed, achieving arthritis remission. ARN induced by tocilizumab was diagnosed, and treatment was swapped to filgotinib monotherapy. Six months later, RN had reduced in size and number, US inflammation had resolved, and arthritis remained in remission.
Case 2
In November 2022, a 64-year-old woman with a one-year history of seropositive non-erosive RA, a tobacco smoker, and a carrier of the HLA-DRB1*0401 allele, was evaluated for inflammatory arthritis in her wrists. She had been on LFN and low-dose methylprednisolone, with previous treatments of hydroxychloroquine and MTX proving ineffective or intolerable. Etanercept was prescribed, but after three months, she reported a dry cough and chest pain despite arthritis improvement. A chest CT scan revealed multiple parenchymal and subpleural lung nodules, 0.5-1.8 cm in diameter, some with central air excavation and peripheral enhancement (Figure 2a). No extra-pulmonary RN were present. A lung biopsy confirmed the presence of RN (Figure 2b). Lung ARN was diagnosed, and etanercept was discontinued, replaced with filgotinib monotherapy. Six months later, the lung nodules had decreased in size and excavation had resolved, with arthritis still in remission.
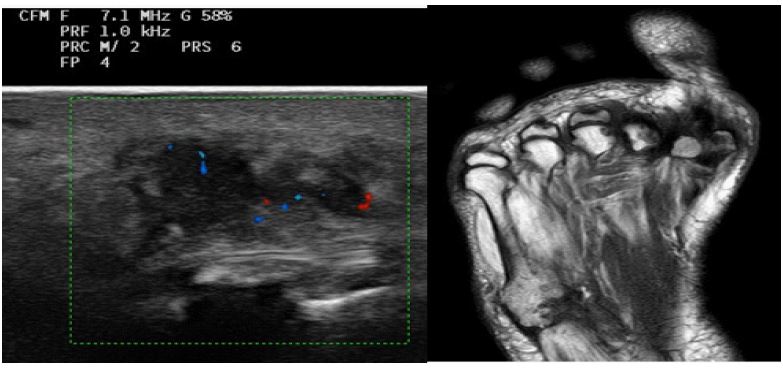
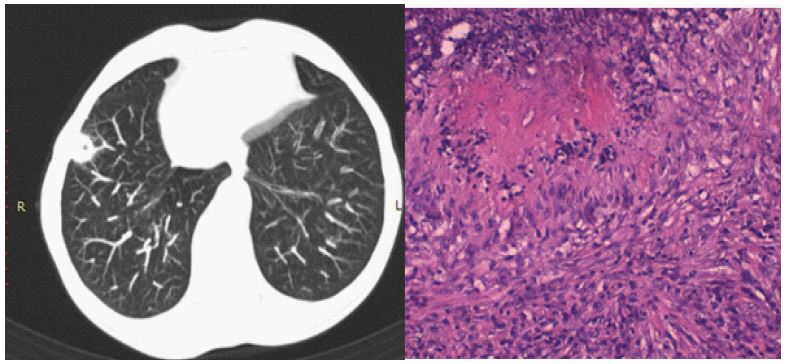
Table 1: Results of literature research inherent to cases of rheumatoid nodules treated with Janus Kinase inhibitors.
| Article | Venerito [26] | V-Mendez [27] | Kondo [28] | Filipescu [29] | Iinuma [30] | Her [31] | Liu [32] |
|---|---|---|---|---|---|---|---|
| Publication year | 2019 | 2020 | 2021 | 2021 | 2022 | 2024 | 2024 |
| Age/sex | 45, F | 58, F | 75, F | 63, F | 70, F | 70, M | 46, F |
| Disease duration* | 1 y | 3 y | 10 y | 17 y | 1 y | - | 1 y |
| Therapies/ duration | MTX/12 m | MTX/ 4 y LFN / 3 yADA/ 3 y | SSz-Tacr/ 1y ETN / 9 y | MTX/ 6y,SSz/ 1 y,LFN/ 2 y | IFX/ 6 m | SSz-steroid/- | MTX/ 1y |
| Combined treatments | - | - | - | MTX 1y | - | LFN 1 y | |
| Predisposing factors | RF/ACPA positivity | RF/ACPA positivity | RF/ACPA positivity | RF/ACPA positivity | - | RF/ACPA positivity | RF/ACPA positivity |
| Site of nodules | lung | hands/feet | lung | lung | hands | lung | lung |
| Preexisting nodules | yes, lung | yes, sc | no | yes, hands | yes, hands | no | no |
| Type of nodules | RN | ARN | ARN | ARN | ARN | RN | ARN |
| Symptoms | no | pain, lossof func-tion, deformities | cough, haemoptysis | fever, dyspnea | pain | cough, dyspnea | no |
| Histology | - | RN | RN | RN | RN | RN | RN |
| Treatment | stop MTXstart BARI | stop ADA, startBARI | stop ETN start ABA,IVCYC and then TOFA | stop LFN, startHCQ, CyS andthen BARI | stop MTX/IFXstart FILGO | stop SSz startTOFA | stop MTX/LFNstart BARI |
| Outcome/time | resolution/4 m | resolution/ 2 y | resolution/- | improvement/ 2 y | reduction insize/ 6 m | reduction insize/ 1 y | reduction insize/ 3-6 m |
ABA: Abatacept; ACPA: Anti-Citrullinated Protein Antibodies; ADA: Adalimumab; ARN: Accelerated Rheumatoid Nodulosis; BARI: Baricitinib; CyS: Ciclosporine; FILGO: Filgotinib; HCQ: Hidroxicloroquine; IFX: Infliximab; IVCYC: Intravenous Cyclophosphamide; LFN: Leflunomide; m: Month; MTX: Methotrexate; RF: Rheumatoid Factor; RN: Rheumatoid Nodule; SSZ: Sulfasalazine; sc: Subcutaneous; Tacr: Tacrolimus; Tofa: Tofacitinib; y: year. *Disease duration before RN or ARN diagnosis.
Discussion
ARN is a subset of RN affecting patients undergoing conventional and biologic disease-modifying anti- rheumatic drugs (c-bDMARDs) therapies for RA. The first description concerning MTX-ARN dates back to 1986 [36], and subsequently ARN was reported in association with multiple c-bDMARDs [4-16]; suggesting the definition of “immunomodulatory agents induced nodulosis” [20].
In our case series, we described two patients with RA who developed ARN shortly after starting biologic bDMARDs – one on tocilizumab and the other on etanercept. Both patients exhibited extensive and complicated nodular lesions, including tissue damage and infection. Notably, neither patient had a history of RN, but both had a genetic predisposition (HLA-DRB1*0401 allele), one was an active smoker—both factors known to increase the risk of ARN [5,19-21]. Despite these risk factors, the development of ARN appeared to be directly related to their bDMARD therapy, as discontinuing these treatments led to significant clinical improvement, strengthened by the swap to JAKi. These findings support the emerging role of JAKi as an efficacious therapeutic option in ARN, consistent with the limited literature on JAKi use in ARN and RN [26-32].
Our review of the literature identified seven published cases of JAKi use in ARN and RN, all of which reported favorable outcomes (Table 1).
These cases, like ours, involved patients with RA who were previously treated with c-bDMARDs (MTX, LFN, anti-TNF agents), highlighting the potential of JAKi as an alternative treatment for ARN. Interestingly, all but one patient were women – despite women being less predisposed to RN formation – suggesting a possible gender influence on JAKi response in RN, most were RF and ACPA positive, with four presenting pre-existing nodules. Our cases add to this body of evidence, providing further support for the efficacy of JAKi in ARN, especially filgotinib, which selectively inhibits pathways involved in RN development [34,35]. The use of JAKi, including filgotinib in monotherapy, appeared to be effective and well-tolerated, with rapid resolution of both subcutaneous and pulmonary nodules, as observed in our patients.
Our review also emphasized the variability of pulmonary ARN, which occurs between <0.4%-32% of RA patients, depending on the method for diagnosis [36]. Pulmonary nodules in ARN are typically asymptomatic unless complications arise, such as hemoptysis, pleural effusion, or pneumothorax, due to cavitation or pleural involvement. In our case, the clinical presentation, characterized by subpleural cavitated nodules, prompted early intervention to prevent serious complications. The use of filgotinib in this setting, though not previously reported in the literature, proved benefit in managing pulmonary nodules, further underscoring its potential place in ARN treatment.
The results from both our case series and the literature review suggest that JAKi, particularly filgotinib, may represent a viable treatment option for ARN. Given the lack of data on JAKi-induced ARN and the apparent protective effect of JAKi against systemic RA manifestations, further studies are needed to clarify their employ in ARN and other extra-articular complications of RA.
References
- Ziffi M. The rheumatoid nodule. Arthritis Rheum. 1990; 33: 761-767.
- Sayah A, English JC 3rd. Rheumatoid arthritis: a review of the cutaneous manifestations. J Am Acad Dermatol. 2005; 53: 191-209.
- Bywaters EG. A variant of rheumatoid arthritis characterized by recurrent digital pad nodules and palmar fasciitis, closely resembling palindromic rheumatism. Ann Rheum Dis. 1949; 8: 2-30.
- Patatanian E, Thompson DF. A review of Methotrexate-Induced Accelerated Nodulosis. Pharmacotherapy. 2022; 22: 9.
- Berkun J, Abou Atta I, Rubinow A, Orbach H, et al. 2756GG genotype of methionine synthase reductase gene is more prevalent in rheumatoid arthritis patients treated with methotrexate and is associated with methotrexate-induced nodulosis. J Rheum. 2007; 34: 1664-9.
- Rozin A, Yigla M, Guralnik L, Keidar Z, Vlodavsky E, Rozenbaum M, Nahir AM, Balbir- Gurman. A. Rheumatoid lung nodulosis and osteopathy associated with leflunomide therapy. Rheumatol. 2006; 25: 384-8.
- Kellet CV, Andino Navarrete R, González Bombardieri S, Manriquez J. Azathioprine-induced accelerated cutaneous and pulmonary nodulosis in a patient with rheumatoid arthritis. An Bras Dermatol. 2015; 90: 162-4.
- Mackley CL, Ostrov BE, Ioffreda MD. Accelerated cutaneous nodulosis during Infliximab therapy in a patient with Rheumatoid Arthritis. J Clin Rheumatology. 2004; 10: 6.
- van Ede A, den Broeder A, Wagenaar M, van Riel P, Creemers MCW. Etanercept-Related Extensive Pulmonary Nodulosis in a Patient with Rheumatoid Arthritis. J of Rheumatology. 2007; 34:1590-2.
- Cunnane G, Warnock M, Fye KH, Daikh DI. Accelerated nodulosis and vasculitis following etanercept therapy for rheumatoid arthritis. Arthritis Rheum 2002; 47:445-9.
- Kekow J, Welte T, Kellner U, Pap T. Development of rheumatoid nodules during anti-tumor necrosis factor alpha therapy with etanercept. Arthritis Rheum 2002; 46:843-4.
- Hubscher O, Re R, Iotti R. Pulmonary rheumatoid nodules in an etanercept-treated patient. Arthritis Rheum 2003; 48:2077-8.
- Toussirot E, Berthelot JM, Pertuiset E, Bouvard B, Gaudin P, Wendling D, et al. Pulmonary Nodulosis and Aseptic Granulomatous Lung Disease Occurring in Patients with Rheumatoid Arthritis Receiving Tumor Necrosis Factor-α-Blocking Agent: A Case Series. The Journal of Rheumatology November. 2009; 36: 2421-2427.
- Watson P, Simler N, Screaton N, Lillicrap M. Management of accelerated pulmonary nodulosis following etanercept therapy in a patient with rheumatoid arthritis. Rheumatology. 2008; 47: 928-9.
- Geetha Wickrematilake. Complicated Rheumatoid Nodules in Lung. Case Reports in Rheumatology. 2020; 2020: 6627244.
- Talotta R, Atzeni F, Batticciotto A, Ditto MC, Gerardi MC, Sarzi-Puttini P. Accelerated subcutaneous nodulosis in patients with rheumatoid arthritis treated with tocilizumab: a case series. J Medical Case Reports. 2018; 12: 154.
- Wikaningrum R, Highton J, Parker A, Coleman M, Hessian PA, Roberts-Thompson PJ, et al. Pathogenic mechanisms in the rheumatoid nodule: comparison of proinflammatory cytokine production and cell adhesion molecule expression in rheumatoid nodules and synovial membranes from the same patient. Arthritis Rheum. 1998; 41: 1783- 97.
- Hessian PA, Highton J, Kean A, et al. Cytokine profile of the rheumatoid nodule suggests that it is a Th1 granuloma. Arthritis Rheum. 2003; 48: 334-338.
- Ahmed SS, Arnett FC, Smith CA, Ahn C, Reveille JD. The HLA DRB1*0401 Allele and the Development of Methotrexate-Induced Accelerated Rheumatoid Nodulosis. A Follow-Up Study of 79 Caucasian Patients with Rheumatoid Arthritis. Medicine. 2001; 80: 271-278.
- Abdwani R, Scuccumarri R, Duffy K, Duffy CM. Nodulosis in systemic onset juvenile idiopathic arthritis: an uncommon event with spontaneous resolution. Pedriatr Dermatol. 2009; 26: 587-91.
- Suzuki A, Morita S, Ohshima M, Minemura N, Suzuki T, Yoshida M, et al. Simultaneous occurrence of accelerated nodulosis in lung, liver, kidneys, and acute exacerbation of interstitial pneumonia in a patient with rheumatoid arthritis: an autopsy case report. BMC Pulm Med. 2022; 22: 10.
- Dash S, Seibold JR, Tiku MI. Successful treatment of methotrexate induced nodulosis with d-penicillamine. J Rheumatol. 1999; 26:1936-1938.
- Abraham Z, Rozembaum M, Rosner I. Colchicine therapy for low-dose-methotrexate-induced accelerated nodulosis in a rheumatoid arthritis patient. J Dermatol. 1999; 26:691-694.
- De Stefano R, Frati E, Nargi F, Menza L. Efficacy of rituximab on pulmonary nodulosis occurring or increasing in patients with rheumatoid arthritis during anti-TNF- α therapy. Clin
- Andres M, Vela P, Romera C. Marked improvement of lung rheumatoid nodules after treatment with tocilizumab. Rheumatology. 2012; 51: 1132-4.
- Venerito V, Lopalco G, Anelli MG, Cacciapaglia F, Iannone F. Tomographic regression of pulmonary rheumatoid nodules under baricitinib therapy. Rheumatology. 2019; 58: 440.
- Valor-Méndez L, Hagen M, Kleyer A, Manger B, Schett G. Massive nodulous lesions on hands and feet in a RA patient and improvement under baricitinib treatment. Rheumatic and musculoskeletal diseases. 2020; 6: e001493.
- Kondo M, Murakawa Y, Honda M, Yanagawa T, Nagasaki M, Moriyama M, et al. A case of rheumatoid arthritis with multiple lung rheumatoid nodules successfully treated with tofacitinib. Mod Rheumatol Case Rep. 2021; 5: 1-5.
- Filipescu IC, Man M, Rednic S. Active rheumatoid arthritis with multiple pulmonary nodules failure to multiple remissive therapy: Which is the solution? Ro J Rheumatol. 2021: 30).
- Iinuma S, Hayashi K, Ishida-Yamamoto A. Accelerated rheumatoid nodulosis resolved after switching to Janus kinase inhibitor therapy. The Journal of Dermatology. 2023; 50: e 98-e99.
- Her M, Park J, Lee SG. A large pulmonary nodule in a rheumatoid arthritis patient treated with tofacitinib. Int J Rheum Dis. 2024; 27: e15013.
- Liu H, Li Q, Long K, Xia O, Ye Y, Wang H, et al. Rheumatoid arthritis with pulmonary accelerated rheumatoid nodules treated by baricitinib: a case-based review. Clin Rheumatology. 2024; 43: 775-784.
- Kremer JM, Lee JK. The safety and efficacy of the use of methotrexate in long-term therapy for rheumatoid arthritis. Arthritis Rheum. 1986; 29: 822-31.
- Szekanecz Z, Buch MH, Schoeman C, Galloway J, Karpouzas GA, Kristensen LE, et al. Efficacy and safety of JAK inhibitors in rheumatoid arthritis: update for the practising clinician. Rev Rheumatol. 2024; 20: 101-115.
- Angelini J, Talotta R, Roncato R, Fornasier G, Barbiero G, Dal Cin L, et al. JAK-Inhibitors for the Treatment of Rheumatoid Arthritis: A Focus on the Present and an Outlook on the Future. Biomolecules. 2020; 10: 1002.
- Yousem SA, Colby TV, Carrington CB. Lung biopsy in rheumatoid arthritis. The American Review of Respiratory Disease. 1985; 131: 770-777.