
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Case report on adult hypertrophic pyloric-stenosis: A rare presentation
Pamathy Gnanaselvam*; Jayaweera SK; Saranga Eshanie Wickramaratne; G Mathivannan; Pirahanthan Karunanithy
Department of Surgery, National Hospital of Sri Lanka, Sri Lanka.
*Corresponding Author : Pamathy Gnanaselvam
Department of Surgery, National Hospital of Sri Lanka, Colombo 10, Sri Lanka.
Email: pamathysha@yahoo.com
Received : Dec 10, 2024
Accepted : Jan 22, 2025
Published : Jan 29, 2025
Archived : www.jcimcr.org
Copyright : © Gnanaselvam P (2025).
Abstract
Idiopathic Hypertrophic Pyloric Stenosis (IHPS) is predominantly a disease in infancy where adult type IHPS is extremely rare. This report is based on 51- year- old female patient diagnosed with AIHPS presented with progressively worsening episodic vomiting, dyspeptic symptoms and constitutional symptoms. Esophagogastroduodenoscopy denoted positive cervix sign. Despite unsuccessful medical management and repeated pyloric dilation, she underwent open pyloromyotomy. This case highlights the importance of considering AIHPS in adults presenting with persistent dyspeptic symptoms and vomiting unresponsive to standard medical therapy. Condition is currently best treated by laparoscopic pyloroplasty.
Keywords: Adult pyloric stenosis; Gastric outlet obstruction; Cervix sign; Pyloroplasty.
Citation: Gnanaselvam P, Jayaweera SK, Wickramaratne SE, Mathivannan G, Karunanithy P. Case report on adult hypertrophic pyloric-stenosis: A rare presentation. J Clin Images Med Case Rep. 2025; 6(1): 3444.
Introduction
Adult Idiopathic Hypertrophic Pyloric Stenosis (AIHPS) is an extremely rare condition, first described by Cruveilhier in 1835 [15]. It is characterized by hypertrophy of the circular muscle fibers of the pyloric canal, leading to gastric outlet obstruction. Most cases of hypertrophic pyloric stenosis in adults are secondary to peptic ulcer disease, malignancy, or inflammatory conditions [10]. However, it is important to differentiate AIHPS from other conditions that can mimic its symptoms, such as Gastrointestinal Stromal Tumors (GISTs) with uncomplicated spindle cell neoplasms which may present with similar clinical features but require different management [5]. The diagnosis of AIHPS is often challenging due to the nonspecific nature of clinical and laboratory findings. Surgical resection followed by histopathological examination is often performed to establish definitive diagnosis and to provide treatment [2].
Case presentation
A 51-year-old Sri Lankan female presented with a three-month history of epigastric pain, along with intermittent projectile vomiting occurring several hours after meals. She had a longstanding history of recurrent dyspeptic symptoms and regurgitation over the past three years, for which she had been treated for Gastroesophageal Reflux Disease (GERD) without significant improvement. Despite being prescribed antiemetic and antacid therapies, her symptoms persisted. Over the course of one year, she experienced significant unintentional weight loss of over 30 kg, with her body weight decreasing to 42 kg and a BMI of 17.5 at the time of her latest presentation.
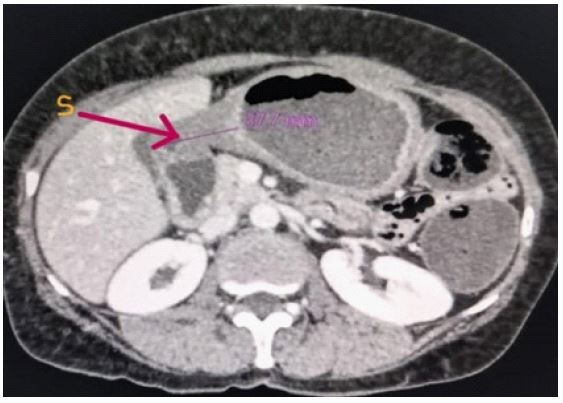
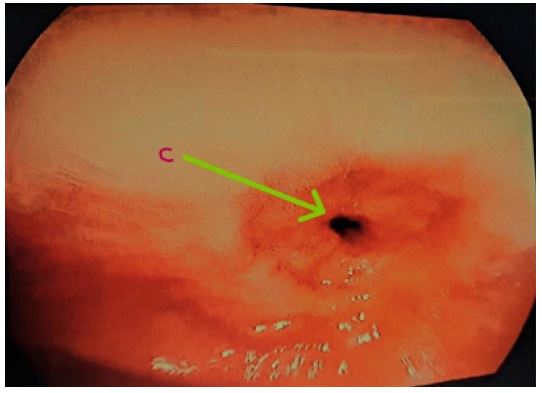
An Esophagogastroduodenoscopy (EGD) revealed a positive cervix sign (Figure 2), a classic finding in pyloric stenosis, and repeated pyloric dilatation was performed three times with limited success. A contrast-enhanced abdominal CT scan showed marked thickening of the pyloric wall (Figure 1), further supporting the suspicion of pyloric stenosis. An endoscopic biopsy of the gastric antrum revealed chronic gastritis, without evidence of malignancy.
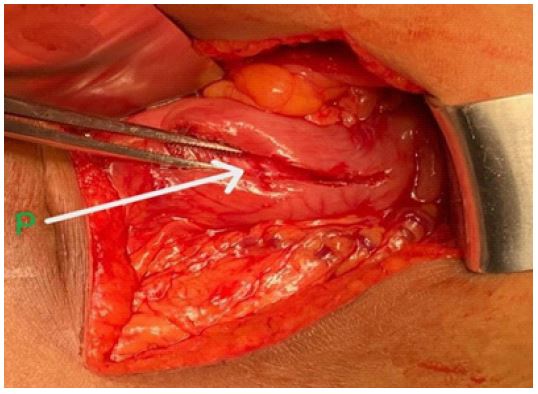
After considering the treatment options, the patient underwent open pyloromyotomy as a definitive surgical intervention (Figure 3). The procedure was uneventful, and the patient experienced no postoperative complications. She was discharged on the third postoperative day and was followed up for one year. During this period, she reported complete resolution of her symptoms and gained approximately 8 kg in weight.
Discussion
Adult pyloric Stenosis is classified as primary & secondary stenosis [1]. Secondary Pyloric Stenosis is much common [2]. Scarring of the distal pylorus and antral region of the stomach due to recurrent peptic ulceration and subsequent fibrosis is considered as the key etiological factor. Other common inflammatory conditions that can be associated are Hypertrophic gastritis (menetrier’s disease), eosinophilic gastritis and Inflammatory bowel diseases affecting the pylorus.
Common malignant conditions associated with secondary pyloric Stenosis [3] included Gastrointestinal Stromal Tumors (GIST), Gastrointestinal Lymphomas including MALT and carcinoid tumors and distal gastric adenocarcinomas. Additionally, Zollinger - Ellison syndrome is associated with excessive gastric acid secretion and subsequent ulceration and glandular hypertrophy causing pyloric stenosis [4] in adults. Mechanical gastric Outlet Obstruction due to locally advanced pancreatic head/ body tumors, Ectopic pancreatic tissue growths, post operative extrinsic adhesions are uncommon causes [5].
Hypertrophic pyloric stenosis without significant predisposing factor is defined as primary or idiopathic. This condition is characterized by hypertrophy and hyperplasia of the pyloric muscle, as observed in histological specimens, mainly composed of fibrofatty tissue. Primary pyloric Stenosis mainly seen in the first- born male child, mainly detected in first few months of life. Adult primary pyloric stenosis is extremely rare. There is few idiopathic hypertrophic pyloric stenosis cases reported worldwide, the majority are middle aged fem ale. Genetics/ familial factors have been proposed in primary pyloric stenosis. Few cases propose a hypothesis in that persistent milder form of hypertrophic pyloric stenosis [6] from infancy can lead to gradual progression of worsening of symptoms.
Considering the clinical presentation of adult hypertrophic pyloric stenosis, the majority presented with episodic non bilious vomiting with Gastric Outlet Obstruction symptoms and mild right hypochondrial/ epigastric pain. Usually, progressive symptoms over few months to years are evident [7]. There might not be definitive palpable lumps in abdominal examination as such of olive sized mass in right hypochondrium typically seen in children. Due to repeated bouts of vomiting and reduced dietary intake, they might be malnourished. In our case she developed significant weight loss and symptoms of undernutrition.
Imaging modalities alone do not provide pathognomonic findings for Adult Idiopathic Hypertrophic Pyloric Stenosis (AIHPS). Barium swallow studies can show delayed transit, while a contrast-enhanced abdominal CT scan might demonstrate pyloric wall thickening, which can assist in diagnosis. Esophagogastroduodenoscopy (EGDS) is essential for diagnosing pyloric stenosis. The “cervix sign,” characterized by a fixed appearance and smooth contours of the pylorus, is both diagnostic and highly suggestive of pyloric stenosis [8]. This sign was observed in our patient on EGDS, where the pyloric wall thickening and cervix sign were present further confirming pylori wall thickening of her CECT.
Macroscopically normal thickness of the pyloric muscle is typically between 3-8 mm. In cases of pyloric stenosis, the muscle can thicken to between 1-3 cm [9]. Histological features of hypertrophy and hyperplasia of the circular muscle layers of the pylorus are considered definitive for diagnosis.
Definitive management for Adult Idiopathic Hypertrophic Pyloric Stenosis (AIHPS) is surgical intervention. Historically, this involved gastric resection and a Billroth I anastomosis. However, the standard approach has shifted to pyloroplasty or pyloromyotomy, either open, laparoscopic, or robotic assisted. The laparoscopic approach is highly effective and safe in current setting [10] with advantages such as reduced postoperative pain, shorter recovery times, and fewer wound complications. Heineke Miculicz surgical pyloroplasty method entails dividing the pylorus in an axial direction with extension of approximately 2cm on the distal stomach & duodenum followed by transverse fashion suture.
Non-surgical options for managing AIHPS include pyloric dilation, which offers temporary relief [11] but has a high recurrence rate. Endoscopic approaches, such as botulinum toxin injections into the pyloric muscle, provide temporary symptom relief through muscle relaxation. Partially covered self-expandable metallic stents have emerged as alternative novel options [12]; however, stent dislodgment can occur over time. A less invasive, flexible endoscopic pyloromyotomy technique using a triangle-tip knife to perform submucosal cutting [13] along the inter muscular propria extending from the pyloric sphincter to the duodenum is available in few centers worldwide. It is proposed that this method is equally effective [14] as laparoscopic approaches.
Conclusion
Adult Idiopathic Hypertrophic Pyloric Stenosis (AIHPS) is an uncommon but important diagnosis that should be considered in adults presenting with recurrent nausea and vomiting that is poorly responsive to antiemetics and acid suppression medications. The “cervix sign” observed during EGDS is a critical diagnostic feature that should not be overlooked. In the Sri Lankan setting, AIHPS is currently best managed with laparoscopic or open pyloromyotomy, providing excellent outcomes in terms of symptom relief and quality of life.
References
- Lin Hsien Ping, Lin Yu-Chiang, Kuo Chen-Yun. Adult idiopathic hypetrophic pyloricstenosis—A case report. Journal of the Formosan Medical Association. 2012.
- Lin HP, Lin YC, Kuo CY. Adult idiopathic hypertrophic pyloric stenosis. J Formos Med Assoc. 2015; 114: 659-662.
- Ger R. Post-Operative Extrinsic Pyloric Stenosis. Br Med J. 1964; 2: 294.
- Choi SJ, Jang YJ, Choe BH, et al. Eosinophilic gastritis with gastric outlet obstruction mimickinginfantile hypertrophic pyloric stenosis. J Pediatr Gastroenterol Nutr. 2014; 59: e9e11.
- Zarineh A, Leon ME, Saad RS, Silverman JF. Idiopathic hypertrophic pyloric stenosis in anadult, apotential mimic of gastric carcinoma. Patholog Res Int. 2010; 2010: 614280.
- Fenwick T. Familial hypertrophic pyloric stenosis. Br Med J. 1953; 2: 12- 14.
- Walsh MH, Quigley PJ. Pyloric stenosis in the dog caused by hypertrophy of the circular muscleof the pylorus. Vet Rec. 1966; 78: 13-15. 18.
- Dye TE, Vidals VG, Lockhart CE, Snider WR. Adult hypertrophic pyloric stenosis. Am Surg. 1979; 45: 478-484.
- Knight CD. Hypertrophic pyloric stenosis in the adult. Ann Surg. 1961; 153: 899- 910.
- Danikas D, Geis WP, Ginalis EM, Gorcey SA, Stratoulias C. Laparoscopic pyloroplasty in idiopathichypertrophic pyloric stenosis in an adult. JSLS. 2000; 4: 173-175.
- Kuwada SK, Alexander GL. Long-term outcome of endoscopic dilation of nonmalignant pyloric stenosis. Gastrointest Endosc. 1995; 41: 15-17.
- Lau JY, Chung SC, Sung JJ, et al. Through-the-scope balloon dilation for pyloric stenosis: longterm results. Gastrointest Endosc. 1996; 43: 98-101.
- Misra SP, Dwivedi M. Long-term follow-up of patients undergoing ballon dilation for benignpyloric stenoses. PRACTICAL GASTRO A Peer Review Journal Endoscopy. 1996; 28: 552-554.
- Solt J, Bajor J, Szabó M, Horváth OP. Long-term results of balloon catheter dilation for benigngastric outlet stenosis. Endoscopy. 2003; 35: 490-495.
- Cruveilhier J. Anatomie Pathologique du Corps Humain. Paris: Bailliere. 1835.